Featured This month
-
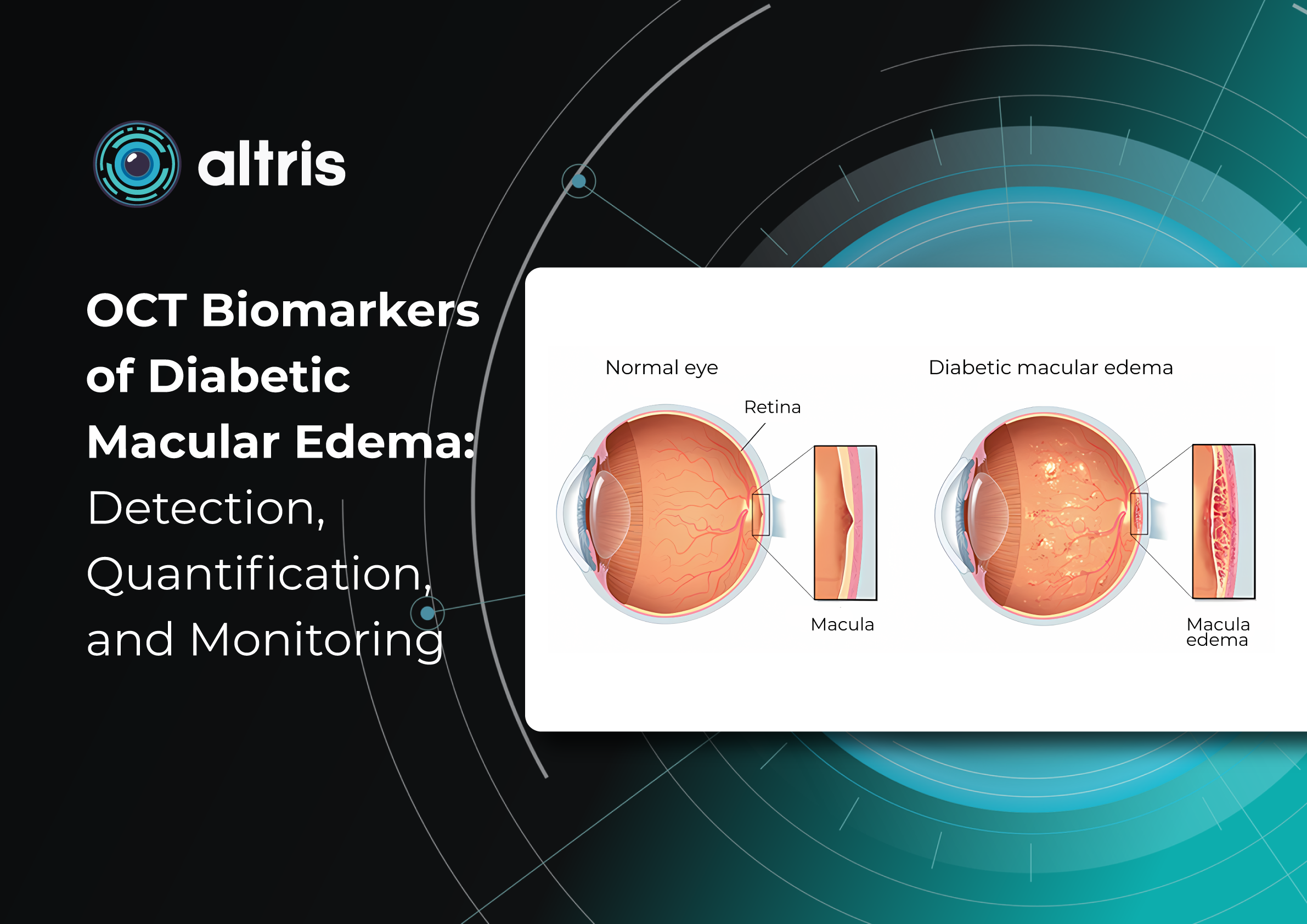
OCT biomarkers in diabetic macular edema: detection, quantification, and monitoring
 Maria Znamenska
5 min.
Maria Znamenska
5 min.Table of Contents
The pathogenesis of OCT biomarkers in diabetic macular edema (DME) is complex and multifactorial. The key mechanism is disruption of the inner blood–retinal barrier resulting from chronic hyperglycemia.
- Introduction. Brief overview of diabetic macular edema (DME)
- Main OCT biomarkers of DME
2.1 Signs of DME on OCT
2.2 Quantitative parameters for monitoring DME on OCT
DME management and patient education: key aspects of the modern approach
ReferencesIntroduction. Brief Overview of Diabetic Macular Edema (DME)
The pathogenesis of OCT biomarkers in diabetic macular edema (DME) is complex and multifactorial. The key mechanism is disruption of the inner blood–retinal barrier resulting from chronic hyperglycemia. This leads to increased vascular permeability, plasma extravasation, and fluid accumulation within the retinal layers. Inflammatory processes, cytokine and growth factor activation—particularly vascular endothelial growth factor (VEGF)—also play an important role by further increasing vascular permeability and sustaining chronic edema. For this reason, DME is now regarded not only as a vascular disorder but also as a neurodegenerative and inflammatory pathology.
Morphologically, DME is characterized by retinal thickening, the formation of intraretinal cystoid spaces, accumulation of subretinal fluid, and progressive photoreceptor damage. Importantly, these structural changes often develop long before the onset of clinical symptoms. A patient may not experience significant visual deterioration, while irreversible changes are already occurring at the microstructural level. This underscores the critical importance of early diagnosis and regular monitoring.
Current clinical guidelines, including those of the American Academy of Ophthalmology, emphasize that the timely detection of DME and the early initiation of treatment significantly improve functional outcomes. However, effective patient management is impossible without precise instrumental monitoring, particularly with optical coherence tomography (OCT), which enables assessment of both the presence and progression of the pathological process.
OCT has become the imaging modality that fundamentally transformed the approach to the diagnosis and treatment of DME. It provides noninvasive visualization of the retina with micron-level resolution, allowing detailed analysis of its layered structure.
Moreover, modern tomographic systems enable a transition from qualitative to quantitative assessment. Measurement of central retinal thickness, lesion area, and other parameters provides objective monitoring of disease progression. This is especially important in the era of personalized medicine, when treatment decisions are based not only on the clinical picture but also on precise numerical indicators.
Thus, modern management of DME cannot be envisioned without the systematic use of OCT and the analysis of its biomarkers. Ophthalmology has progressed from simply detecting edema to achieving a deeper understanding of microstructural changes and their clinical significance.
The aim of this article is to summarize current evidence on OCT biomarkers of diabetic macular edema, their roles in detection, quantitative assessment, and disease monitoring, and the practical aspects of their use in clinical practice to optimize patient management.
2. Main OCT Biomarkers in DME
The modern approach to DME is based on a fundamentally new understanding of OCT’s role. OCT biomarkers in DME enable not only assessment of fluid presence but also determination of its type, localization, severity, and impact on key functional structures, particularly the photoreceptors. This is critically important because DME may have different pathogenic mechanisms across patients, ranging from vascular and inflammatory processes to a predominantly tractional component.
Particular attention should be paid to the role of OCT biomarkers in predicting the course of DME and treatment response. Features such as disorganization of the retinal inner layers (DRIL), the condition of the ellipsoid zone, and the presence of hyperreflective foci are now considered important indicators for predicting disease progression and functional outcomes. These biomarkers enable clinicians to anticipate which patients are more likely to respond favorably to anti-VEGF therapy and in which cases a less favourable visual outcome should be expected.
Each structural element observed on an OCT scan carries its own clinical significance. These findings allow the physician to answer several key clinical questions:
- how active the disease process is,
- whether the condition is acute or chronic,
- which structures have already undergone irreversible changes,
- which pathogenic mechanism predominates,
- and, most importantly, what the likely therapeutic response will be.
Thus, OCT interpretation extends far beyond simple visual assessment. It becomes an analytical process in which the clinician integrates morphological features with quantitative measurements and the patient’s clinical data.
According to current international recommendations, no single parameter—such as central retinal thickness—can be sufficient for clinical decision-making. Instead, analysis of a combination of morphological patterns, quantitative indicators, and their temporal changes is recommended.
The transition from static assessment to dynamic monitoring is particularly important via OCT biomarkers in dme. The rate of change, stability, or progression of individual biomarkers is often more informative than their absolute values. For example, a slight but persistent increase in intraretinal fluid may have greater clinical significance than a single high retinal thickness measurement.
In addition, modern technologies have considerably expanded the capabilities of OCT analysis. The use of automated retinal layer segmentation, quantitative fluid volume assessment, and artificial intelligence algorithms helps reduce subjective interpretation and improve the reproducibility of results. This is especially important both in clinical practice and in scientific research, where accuracy and standardization are essential.
In summary, the contemporary concept of OCT biomarkers in DME is based on three interconnected levels of analysis:
- Morphological level — identification of structural changes and edema type.
- Quantitative level — measurement of retinal thickness, fluid volume, and lesion area.
- Prognostic level — assessment of the risk of progression and treatment response.
It is precisely this multilevel evaluation that enables a transition from standardized treatment protocols to a personalized approach, in which the therapeutic strategy is determined by each patient’s OCT biomarker profile.

2.1 OCT Features of Diabetic Macular Edema (DME)
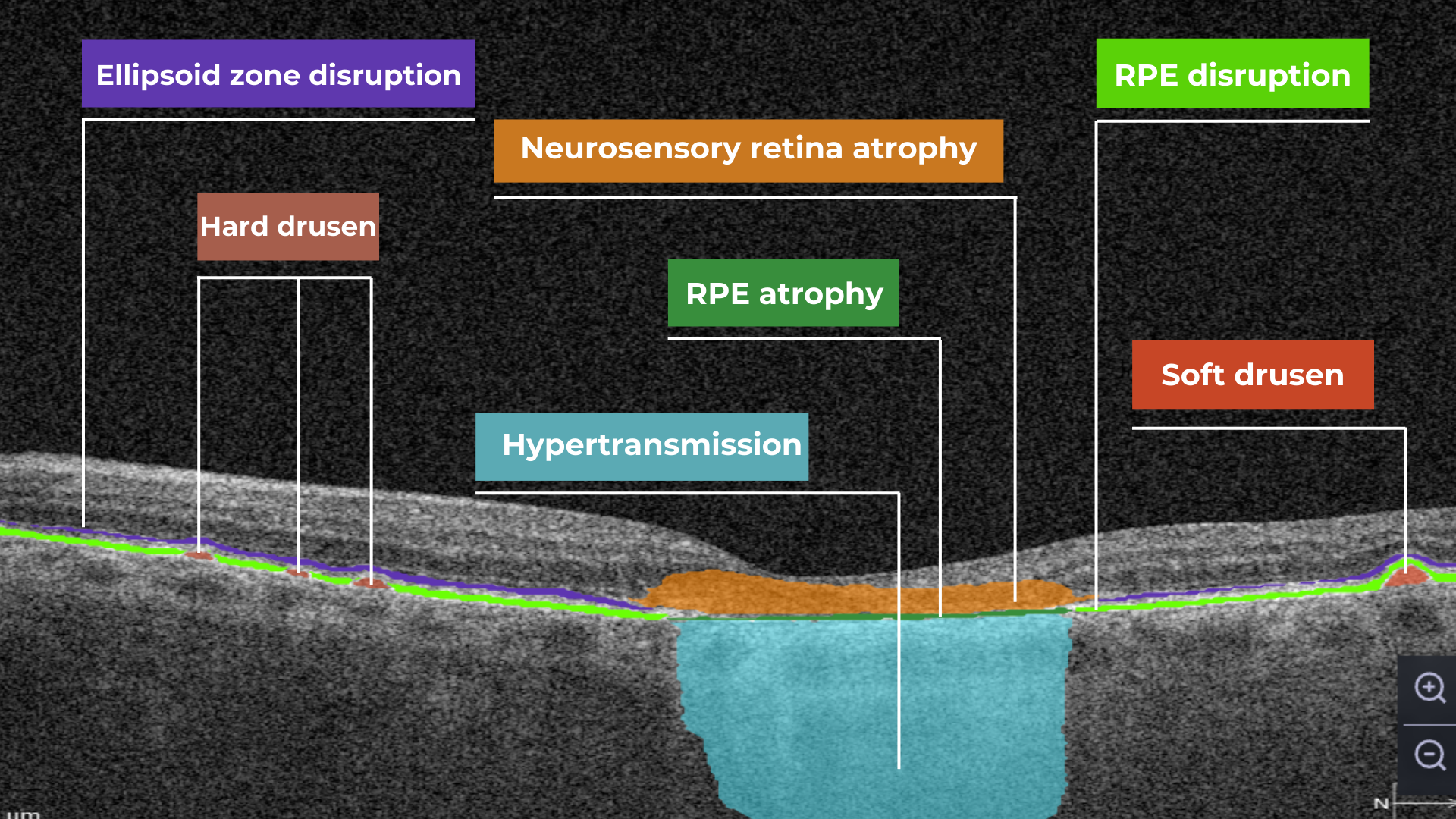
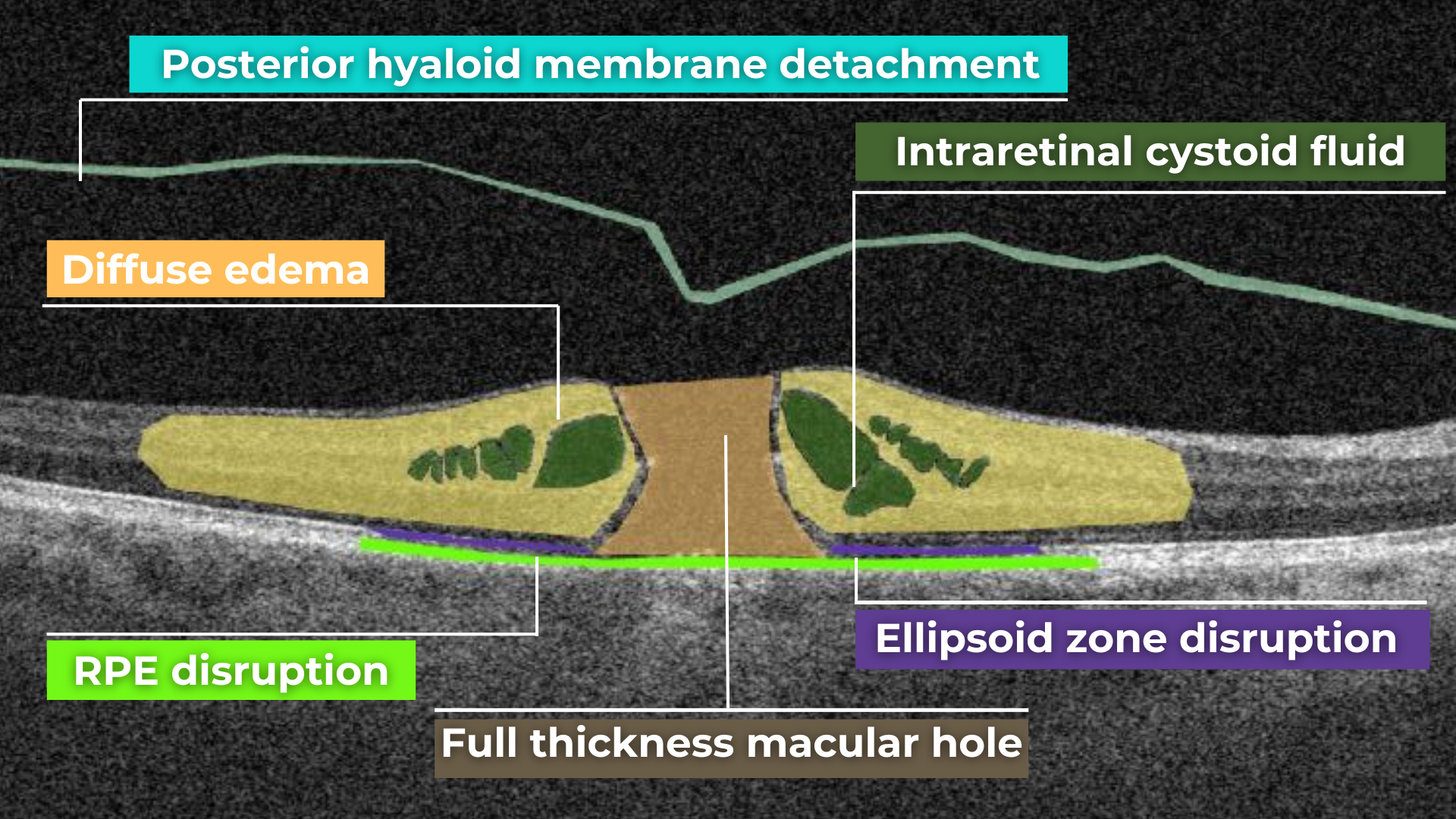
There are several distinct OCT patterns associated with DME, including diffuse retinal thickening, cystoid macular edema (intraretinal cystic spaces), and serous retinal detachment (subretinal fluid).
1. Diffuse retinal thickening
This is characterized by a uniform increase in macular thickness, resulting from fluid accumulation in the extracellular space of the neurosensory retina due to disruption of the inner blood–retinal barrier and an imbalance between fluid leakage and the resorptive capacity of the retinal pigment epithelium (RPE).
When cystic spaces are present, their diameter must not exceed 50 μm; otherwise, the edema is classified as cystoid.
In chronic edema (lasting more than 6–9 months), irreversible photoreceptor damage may occur, along with the development of retinal atrophy.
Key features:
- may be the only finding in early stages
- requires careful quantitative assessment (central retinal thickness, CRT measurement)
- Macular thickness dynamics are an important biomarker of treatment efficacy
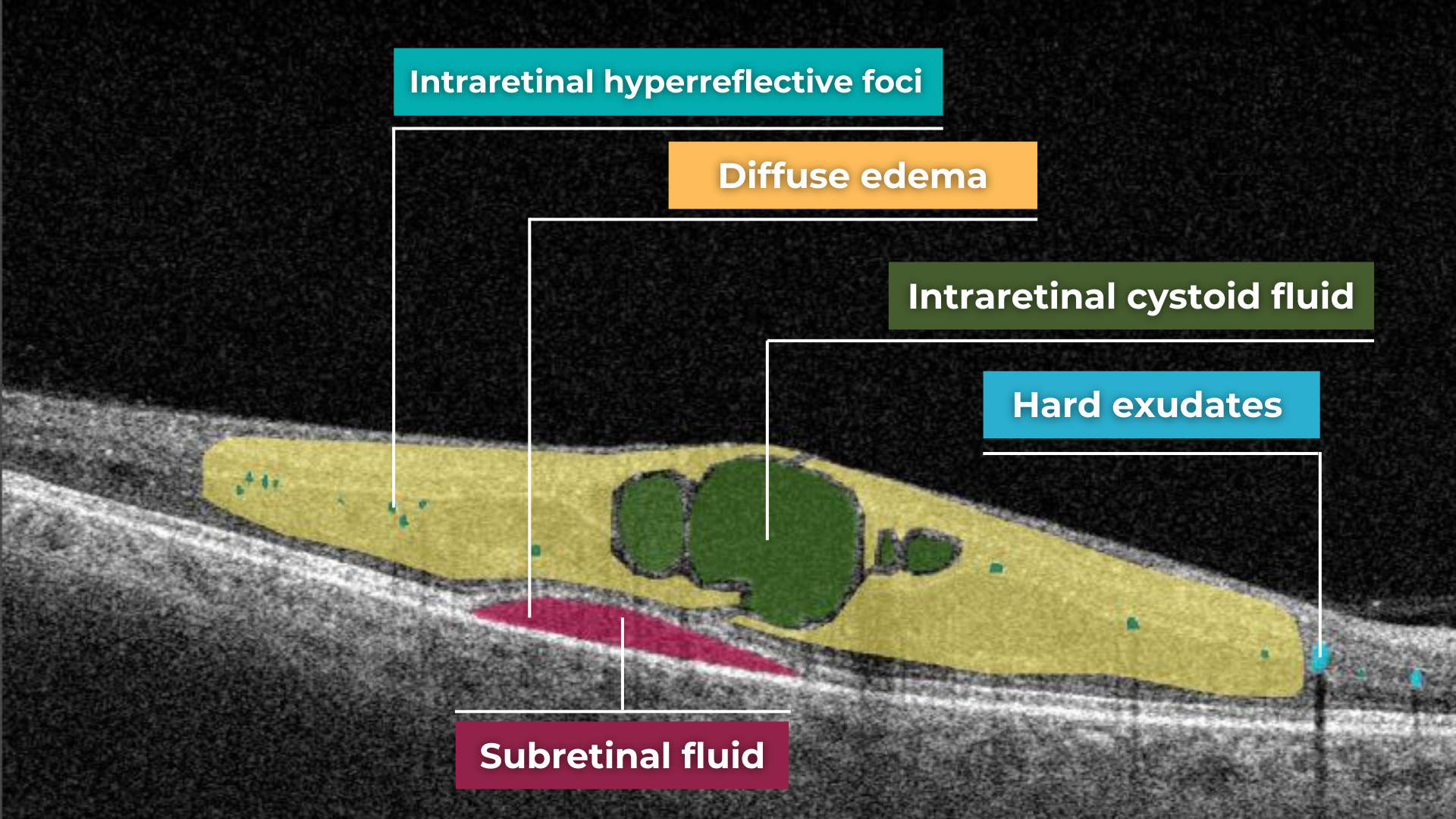
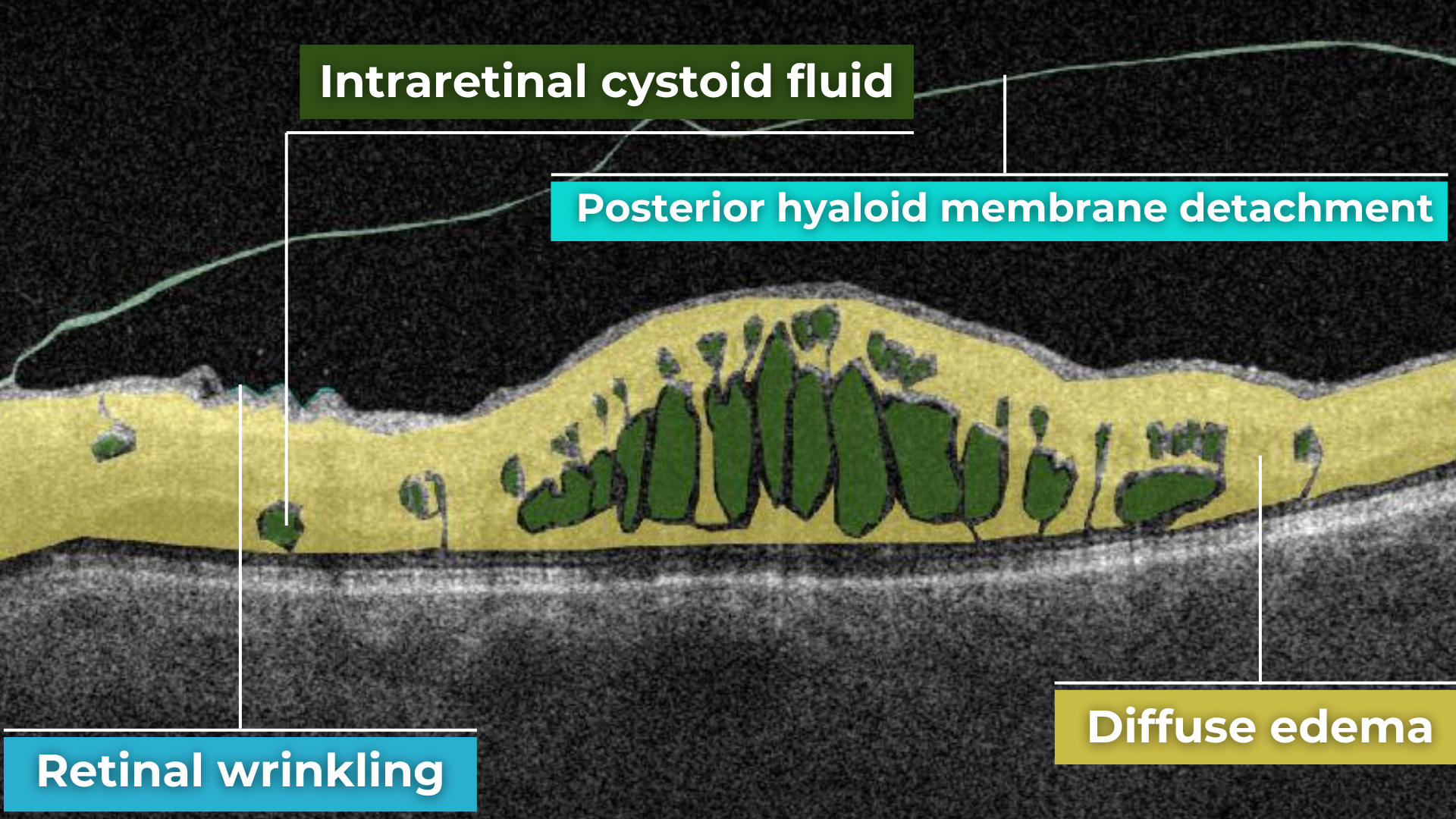
2. Cystoid macular edema (intraretinal cystic spaces)
This is a key structural marker of DME. On OCT, it appears as hyporeflective, round or oval cavities, predominantly located in the inner nuclear layer (INL) and the outer plexiform layer (OPL).
Clinical significance:
- reflects vascular hyperpermeability
- indicates active edema
- large and confluent cysts may suggest a chronic process and are associated with a worse functional prognosis
Long-standing cysts can lead to mechanical stretching of retinal tissue and secondary photoreceptor damage.
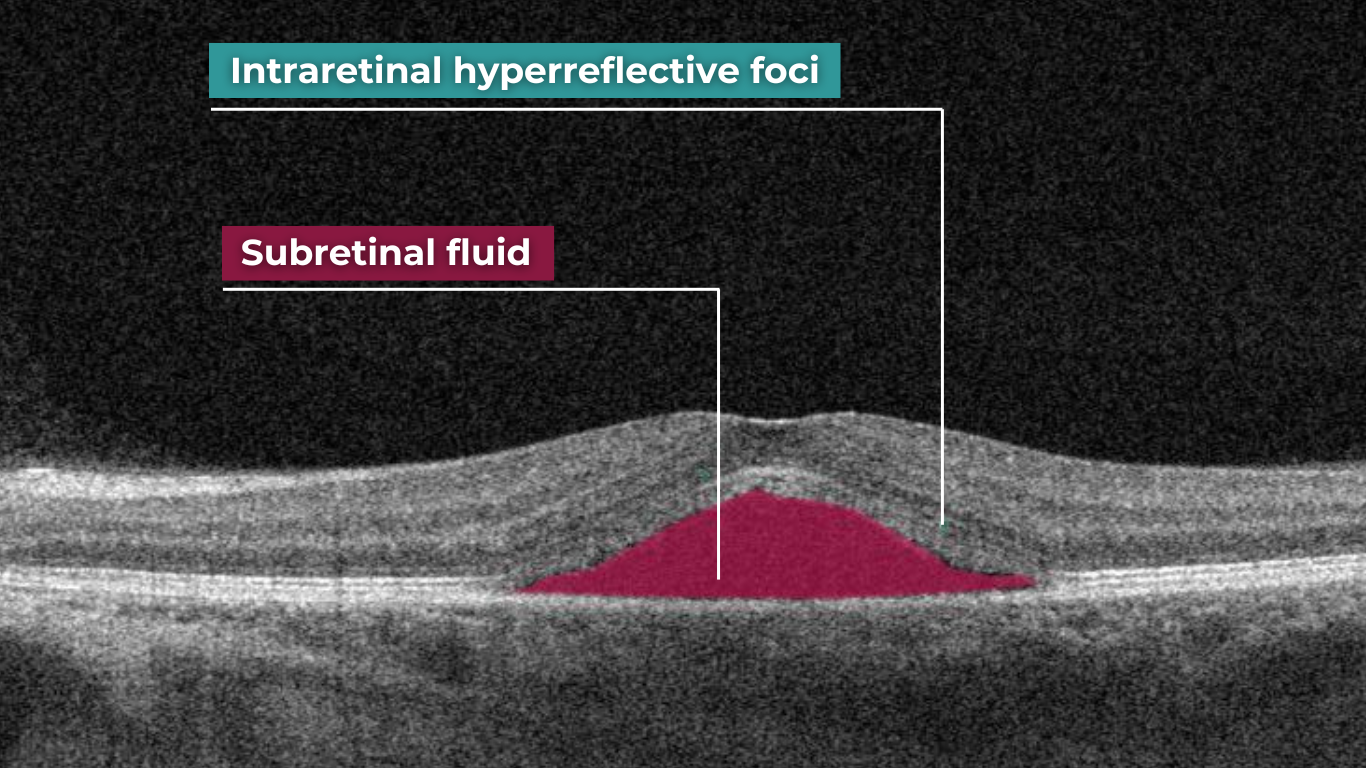
3. Serous retinal detachment (subretinal fluid)
Subretinal fluid refers to the accumulation of fluid between the neurosensory retina and the retinal pigment epithelium (RPE).
On OCT, it appears as a hyporeflective space above the RPE and is associated with neurosensory retinal detachment.
Clinical interpretation:
- may be a marker of active disease
- in some cases is associated with a better response to anti-VEGF therapy
- causes less photoreceptor damage than chronic intraretinal cysts
Although subretinal fluid is generally associated with a relatively better visual prognosis, its presence requires careful monitoring and should be considered when planning anti-VEGF treatment.
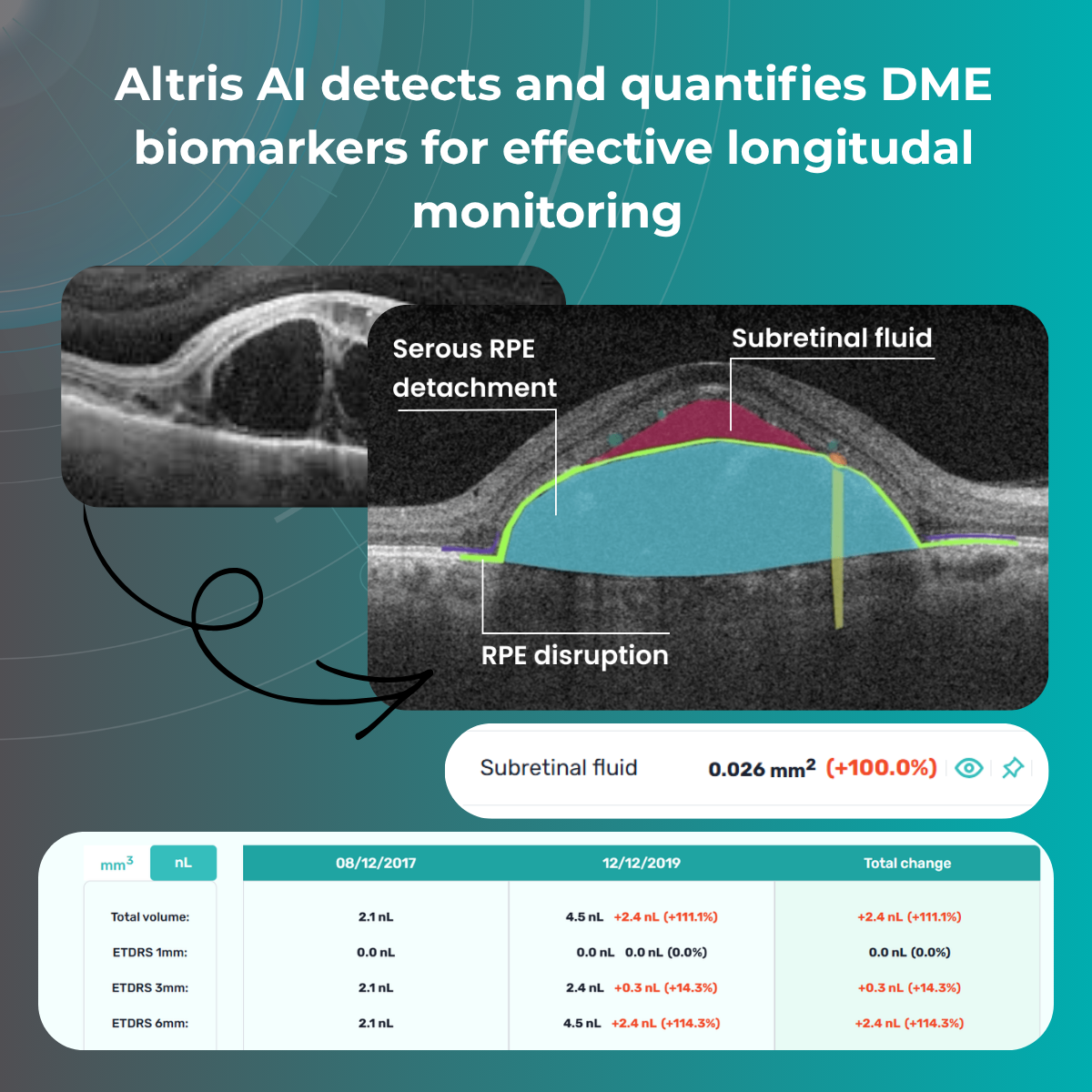
2.2 Quantitative parameters for monitoring DME on OCT
After morphological assessment, the next step is quantitative analysis. Currently, several key quantitative parameters can be obtained:
- Central retinal thickness (CRT) – the most widely used parameter
- Macular volume
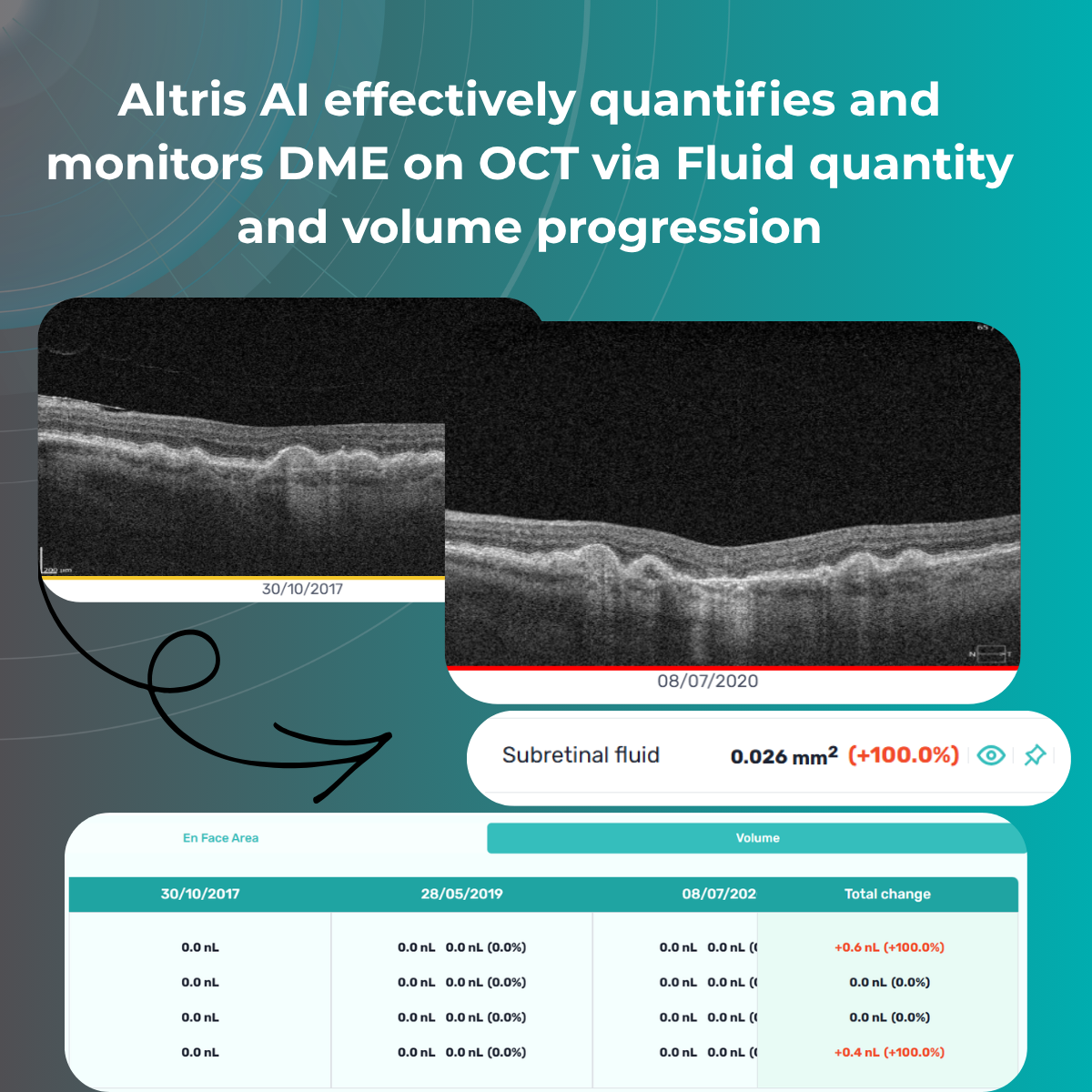
- Fluid quantity and volume
These measurements enable precise monitoring of treatment response and help guide decisions regarding injection intervals.
3. Management of DME and patient education: key aspects of the modern approach
Modern management of diabetic macular edema (DME) is based on a comprehensive, personalized strategy in which OCT plays a central role. Today, therapeutic decisions are influenced by the morphological type of edema, disease activity, integrity of neurosensory retinal structures, individual patient characteristics, comorbidities, and prognostic biomarkers.
A key principle of the contemporary approach is the integration of structural OCT biomarkers in DME into clinical decision-making. These biomarkers not only help determine whether treatment is necessary, but also assist in selecting the optimal therapeutic modality, assessing response, and timely adjustment of management strategy.
Additional factors influencing therapy selection include:
- Presence of disorganization of the retinal inner layers (DRIL) and disruption of the ellipsoid zone (EZ)
- Response to previous treatments
- Systemic comorbidities (renal impairment, hypertension, adherence/compliance issues)
Treatment
Anti-VEGF therapy
Anti-VEGF agents (aflibercept, ranibizumab, bevacizumab) remain the first-line treatment for DME, as they directly target the key pathogenic mechanism—vascular hyperpermeability.
Newer agents with extended durability are emerging, including implantable drug delivery systems.
However, not all patients respond equally to anti-VEGF therapy. Therefore, OCT biomarker analysis is crucial: for example, a predominance of intraretinal cystic changes is usually associated with a good response to anti-VEGF, whereas a high number of hyperreflective foci or signs of chronic edema may indicate a significant inflammatory component and support consideration of steroid therapy.
Intravitreal corticosteroid implants
Steroids are used in cases of chronic and refractory DME, insufficient response to anti-VEGF therapy, and in patients with a pro-inflammatory phenotype.
Laser therapy
Although laser treatment has become less central in current practice, it remains useful in selected clinical scenarios. Subthreshold micropulse laser is more commonly used in patients with focal edema without involvement of the foveal center.
Thus, treatment decisions today are no longer universal; they are based on an individualized OCT-based patient profile.
Role of OCT in treatment
OCT accompanies the patient throughout all stages of treatment and performs several key functions:
- determination of indications for initiating therapy (presence of fluid, macular thickening, involvement of the foveal region)
- assessment of treatment response (reduction of fluid, normalization of thickness, structural restoration)
- detection of resistance or partial response
- optimization of injection intervals (treat-and-extend or pro re nata strategies)
A particularly important aspect is that OCT can detect subclinical changes. For example, minimal fluid accumulation may appear before any subjective deterioration in vision. This enables timely treatment adjustments and the prevention of functional loss.
In addition, OCT helps avoid both under- and overtreatment. In patients with a stable anatomical profile and no fluid, injection intervals can be gradually extended, reducing the burden on both the patient and the healthcare system.

Monitoring
The frequency of follow-up depends on disease stage and activity:
- active treatment phase – monthly visits with OCT control
- stabilization phase – every 2–4 months
- long-term follow-up – individualized, depending on recurrence risk and associated risk factors
It is important to emphasize that monitoring must remain regular even in the absence of symptoms. DME can progress asymptomatically, and only OCT allows objective assessment of retinal status.
Dynamic follow-up is critical: comparison of sequential scans provides the most valuable information about disease progression.
What is important to explain to the patient
Effective management of DME is not possible without active patient participation; therefore, communication is a key component of treatment.
The patient must clearly understand that:
- DME is a chronic condition requiring long-term monitoring
- treatment aims to stabilize and slow disease progression, not always to fully restore vision
- interruption of therapy without medical advice may lead to deterioration
- regular visits and OCT monitoring are critical, even if vision appears stable
It is especially important to explain the role of OCT to patients. Showing scans and explaining changes significantly improves treatment adherence.
Lifestyle and systemic control
Since diabetic macular edema (DME) is a complication of a systemic disease, control of the patient’s overall health is of critical importance.
Key recommendations include:
- optimal glycemic control
- blood pressure management
- correction of lipid profile
- healthy diet rich in antioxidants
- regular physical activity
- smoking cessation

Psychological aspects and treatment adherence
DME often follows a long and fluctuating course, which may lead to treatment fatigue or reduced motivation in patients. Many patients underestimate the severity of the condition, especially in early stages when visual acuity is still preserved.
In this context, OCT becomes not only a diagnostic tool but also a communication instrument. Visualization of pathological changes helps patients better understand the disease and the necessity of treatment.
Establishing a partnership between physician and patient is essential for successful long-term management.
Conclusion
OCT biomarkers in DME now allow not only precise diagnosis but also an approach that goes far beyond traditional retinal assessment. Thanks to its high resolution and ability to visualize microstructural changes, OCT enables the detection of subtle abnormalities before clinically significant symptoms appear. This opens the way to a new level of patient management—shifting from descriptive assessment to quantitative evaluation of pathological changes, their dynamics, and treatment response. Furthermore, OCT biomarker analysis allows prediction of disease course, identification of progression risk, and individualization of therapeutic strategies for each patient.
Modern DME management is not just diagnosis and treatment, but a comprehensive clinical decision-making system based on objective, standardized data. There is a clear shift from subjective interpretation of fundus changes to structured analytics, where every parameter matters: retinal thickness, presence of intra- or subretinal fluid, status of outer retinal layers, and macular architectural disruption. OCT has become the key tool transforming clinical practice, making it more precise, reproducible, and evidence-based. It allows clinicians not only to confirm the presence of pathology but also to better understand its nature, activity, and potential reversibility.
Ultimately, effective DME management today is the result of synergy between modern imaging technologies, clinical reasoning, and active patient engagement. Proper interpretation of OCT images must be integrated into the overall clinical picture, taking into account systemic factors, diabetes duration, and individual patient characteristics. In this process, OCT acts as a central link—a bridge between diagnosis and treatment—uniting all oct biomarkers in diabetic macular edema components into a coherent clinical system. This approach leads to better functional outcomes, preservation of vision, and significant long-term improvement in patients’ quality of life.
FAQ
1. How can AI help detect OCT biomarkers in DME?
AI can automatically identify key OCT biomarkers such as intraretinal fluid, subretinal fluid, hyperreflective foci, and retinal layer disruptions, helping clinicians detect disease activity faster and more consistently.
2. Why is quantitative biomarker analysis important in DME?
Quantification enables objective measurement of biomarker volume, area, and progression over time, supporting treatment decisions, therapy response assessment, and longitudinal patient monitoring.
3. Which OCT biomarkers are most relevant for monitoring DME progression?
Commonly monitored biomarkers include intraretinal fluid (IRF), subretinal fluid (SRF), hyperreflective foci (HRF), disorganization of retinal inner layers (DRIL), and ellipsoid zone disruption.
4. How can automated OCT analysis improve clinical workflow?
Automated analysis reduces manual interpretation time, improves reproducibility, standardizes reporting, and helps clinicians prioritize patients who may require closer follow-up or treatment adjustments.
References
- https://pubmed.ncbi.nlm.nih.gov/38460657/
- https://brief.euretina.org/research/association-of-retinal-oct-biomarkers-with-reading-performance-in-patients-with-diabetic-macular-edema-dme
- https://www.mdpi.com/2075-4418/14/1/76
- https://www.sciencedirect.com/science/article/pii/S1572100024000814
- https://link.springer.com/article/10.1186/s40942-023-00473-w
- https://www.medscape.com/viewarticle/1001580
- https://www.cureus.com/articles/227801-innovations-in-diabetic-macular-edema-management-a-comprehensive-review-of-automated-quantification-and-anti-vascular-endothelial-growth-factor-intervention#!/
-
RWE in Ophthalmology: Challenges of Collection and Processing
Maria Znamenska
3 min.Pharma has no shortage of data in ophthalmology—EHRs, imaging repositories, claims, registries—but the industry still faces a persistent RWE gap when it comes to turning that data into commercially actionable insight.
This gap becomes especially critical in the context of modern ophthalmic therapies, where timing, disease stage, and adherence directly impact outcomes—and, by extension, market performance. Without precise, scalable ways to identify eligible patients (e.g., early-stage AMD, DME with specific biomarkers), commercial teams are left relying on proxies or delayed claims data. At the same time, tracking real-world outcomes remains reactive and retrospective, limiting the ability to support value-based narratives, optimize field strategy, or respond dynamically to physician behavior.
For commercial and market access leaders, closing the RWE gap is no longer a “data strategy” initiative—it’s a growth imperative. The organizations that will lead are those that move beyond passive data aggregation toward active, AI-driven interpretation of multimodal ophthalmic data, enabling near real-time patient identification and outcome tracking. This shift not only strengthens evidence generation but directly translates into sharper targeting, more credible value communication, and ultimately, stronger adoption curves in an increasingly competitive therapeutic landscape.

RWE Key Components
Real-world evidence (RWE) in ophthalmology is fundamentally multimodal—it emerges from the combination of
- OCT imaging,
- clinical metrics,
- treatment patterns,
- and patient context over time.
When these components are connected, they move beyond descriptive data and become decision-grade insight for commercial, medical, and market access teams.
Imaging (OCT): the gold mine of RWE
OCT is the anchor, but only when integrated with outcomes, treatment data, and longitudinal context does it unlock its full commercial value—turning raw data into actionable RWE that can directly shape strategy and growth.
Leverage data from past or ongoing clinical trials with the ability to standardize it within a unified ecosystem. OCT segmentation model can enable you to extract robust, clinically meaningful insights from your trial data to:
- Gain a deeper understanding of patient responses to treatments by characterizing disease progression and outcomes over time.
- Segment patient populations into subgroups to evaluate biomarker-driven profiles and build predictive analytics—helping streamline future trials by refining endpoints and optimizing inclusion and exclusion criteria.
All that, as well as to build one of the most extensive and comprehensive real-world evidence (RWE) databases in ophthalmology may be quite possible within one OCT-vendor neutral data analysis platform ecosystem.
Clinical outcomes: functional reality
Clinical measures—most notably visual acuity (VA), intraocular pressure, and physician-reported assessments—represent the functional impact of disease and treatment. These endpoints are still central to regulatory and commercial narratives, but in isolation they are often lagging indicators. By the time vision declines, disease progression may already be advanced. When paired with imaging, however, clinical outcomes provide the critical link between anatomical change and patient benefit, strengthening real-world value stories and payer communication.
RWE delivers critical insights into how therapies perform in routine clinical practice—such as healthcare outcomes, treatment adherence, and protocol efficiency—often revealing patterns that differ from those observed in controlled clinical trials.

Treatment data: what actually happens in practice
Treatment data captures real-world behavior—which therapies are used, dosing frequency, switching patterns, and adherence. This is where the gap between clinical trial protocols and actual practice becomes visible. For commercial teams, this layer reveals drop-off points, under-treatment, and competitive dynamics at a granular level. When combined with OCT and outcomes, this approach makes it possible to understand not just what is happening but why—for example, whether discontinuation is driven by lack of response, disease stabilization, or operational constraints.
OCT segmentation enables high-throughput processing and deep interrogation of large-scale datasets, enhancing the interpretation of real-world data. It can validate existing assumptions, uncover new patterns, and support hypothesis generation and testing. This analysis provides a clearer view of treatment efficacy and safety, disease progression in real-world settings, and a more precise understanding of target patient populations.
Demographics and patient context
Demographics (age, gender, geography) and broader patient context (comorbidities, access to care) provide the segmentation layer for RWE. These factors influence disease prevalence, treatment eligibility, and adherence patterns. While less granular than imaging, they are essential for market sizing, targeting, and equity considerations, helping commercial leaders understand where the highest-value opportunities—and barriers—exist across populations.
Data analysis includes population-level distributions of retinal layer thickness and fluid volumes; longitudinal tracking of layer and fluid changes over time; and assessment of retinal layer attenuation/loss (depletion maps) and atrophic regions (Figure 2), among other endpoints.
Longitudinal progression: the real differentiator
The true power of RWE lies in its longitudinal nature—tracking how patients evolve over time across imaging, outcomes, and treatment. This enables identification of disease trajectories, early signals of response or non-response, and optimal intervention windows. For pharma decision-makers, longitudinal RWE transforms static snapshots into predictive insight, supporting earlier intervention strategies, more precise patient journeys, and stronger, evidence-backed differentiation in crowded markets.
The Core Problem
There are core RWE problems worth mentioning. pay attention to the following bottlenecks: fragmented data, unstructured imaging, lack of standardization, and broken longitudinal tracking.
- Fragmented data: Patient information is dispersed across multiple systems, limiting the ability to generate a unified, comprehensive view.
- Unstructured imaging: Large volumes of imaging data, such as OCT scans, remain unstructured and difficult to analyze at scale.
- Lack of standardization: Variability in data formats and clinical protocols hinders consistent analysis and comparison.
- Broken longitudinal tracking: Incomplete or disconnected patient timelines prevent accurate assessment of disease progression and treatment outcomes over time.
The core issue isn’t volume; it’s fragmentation and lack of standardization. OCT scans sit in one system, visual acuity in another, treatment histories elsewhere, often unstructured or inconsistently coded. As a result, even well-resourced teams struggle to answer seemingly simple questions like: Who are the untreated but eligible patients? or Which cohorts are actually benefiting from therapy in real-world settings?
However, AI is transforming the RWE in ophthalmology research to:
- Design smarter, biomarker-driven trials
- Estimate disease burden and patient volumes
- Track outcomes, safety, and progression
- Strengthen regulatory and market access strategies
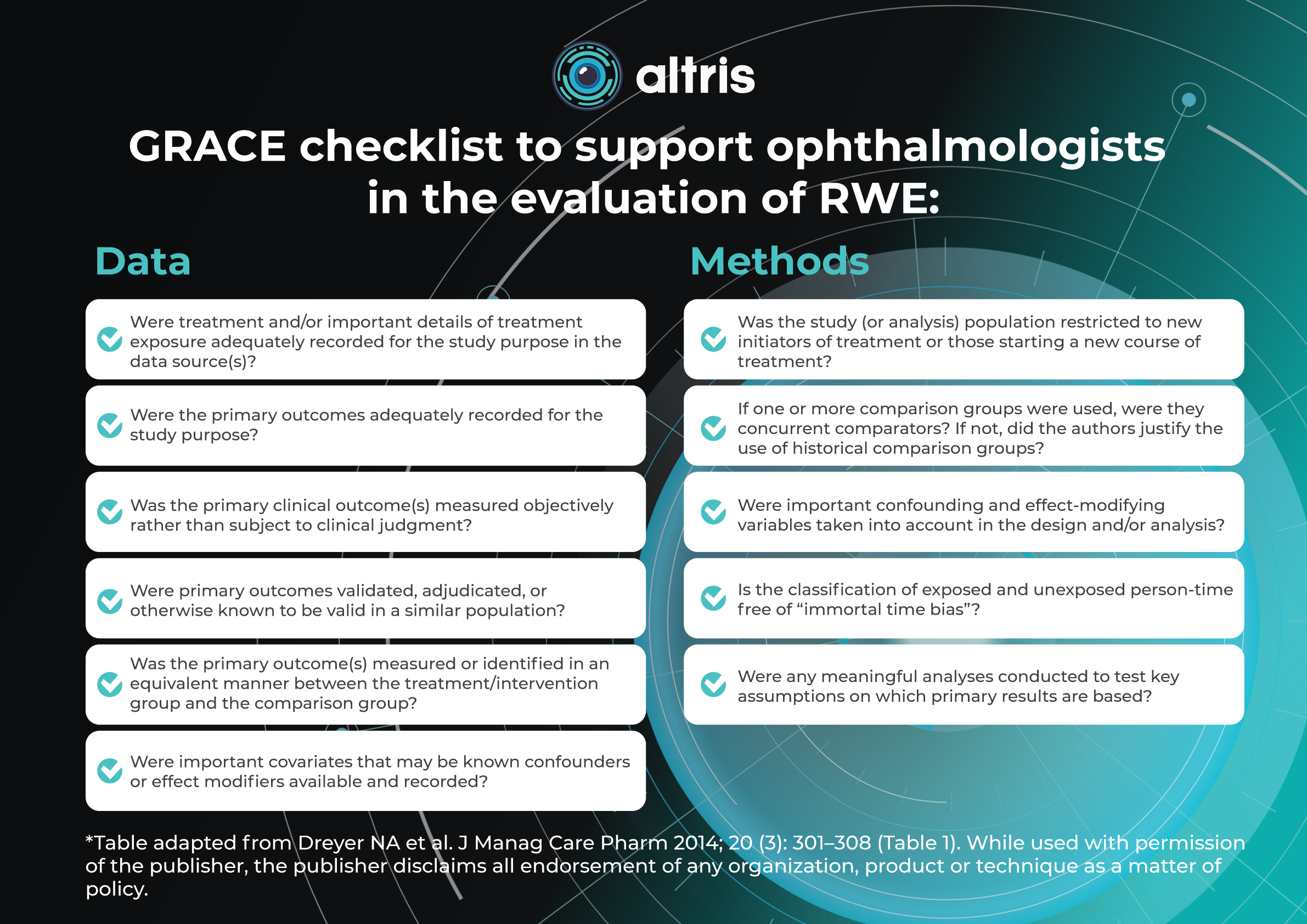
Resources to aid ophthalmologists in evaluating the quality of RWE are available, such as the Good Research for Comparative Effectiveness (GRACE) principles, which can support the evaluation of observational comparative effectiveness studies.
GRACE checklist to support ophthalmologists in the evaluation of RWE:
Data Methods ✓ Were treatment and/or important details of treatment exposure adequately recorded for the study purpose in the data source(s)? ✓ Was the study (or analysis) population restricted to new initiators of treatment or those starting a new course of treatment? ✓ Were the primary outcomes adequately recorded for the study purpose? ✓ If one or more comparison groups were used, were they concurrent comparators? If not, did the authors justify the use of historical comparison groups? ✓ Was the primary clinical outcome(s) measured objectively rather than subject to clinical judgment? ✓ Were important confounding and effect-modifying variables taken into account in the design and/or analysis? ✓ Were primary outcomes validated, adjudicated, or otherwise known to be valid in a similar population? ✓ Is the classification of exposed and unexposed person-time free of “immortal time bias”? ✓ Was the primary outcome(s) measured or identified in an equivalent manner between the treatment/intervention group and the comparison group? ✓ Were any meaningful analyses conducted to test key assumptions on which primary results are based? ✓ Were important covariates that may be known confounders or effect modifiers available and recorded? *Table adapted from Dreyer NA et al. J Manag Care Pharm 2014; 20 (3): 301–308 (Table 1). While used with permission of the publisher, the publisher disclaims all endorsement of any organization, product or technique as a matter of policy.
Why Imaging Is Critical?
OCT is a stepping stone to understanding Geographic Atrophy. Since the approval of the first therapy targeting geographic atrophy in early 2023, interest in the disease has increased dramatically. At the same time, a growing number of clinical trials are underway, evaluating the safety and efficacy of multiple investigational compounds.
Imaging—particularly OCT (optical coherence tomography)—is the backbone of meaningful real-world evidence in retinal disease, because it captures what clinical codes and claims data simply cannot: anatomical change over time. Without structured OCT data, RWE becomes fragmented and largely inferential, relying on indirect proxies like treatment patterns or visual acuity alone. This creates a major blind spot in understanding disease progression, especially in chronic degenerative conditions where structural deterioration often precedes functional loss.
In geographic atrophy (GA), this gap is especially critical for therapies such as Syfovre (pegcetacoplan) and Izervay (avacincaptad pegol). These treatments are designed to slow structural progression, not just improve symptoms, meaning their real-world impact can only be properly assessed through consistent, longitudinal imaging markers—lesion growth, retinal layer integrity, and atrophy expansion. When OCT data is unstructured or missing, it becomes impossible to reliably track these anatomical endpoints across time and across care settings.
As a result, RWE datasets without standardized OCT integration fail to support robust patient journey reconstruction, dilute treatment effect signals, and limit the ability to identify responders vs non-responders. For pharma and clinical stakeholders, this means missed opportunities to demonstrate value, optimize patient selection, and build predictive models that depend on continuous structural imaging rather than episodic clinical snapshots.
The Way Forward
AI-driven structuring of imaging data is emerging as the missing link between raw clinical information and truly actionable real-world evidence (RWE). In ophthalmology, vast volumes of OCT scans remain underutilized because they are stored as unstructured images, making large-scale analysis slow, inconsistent, and often impractical.
By applying advanced algorithms to automatically segment retinal layers, detect biomarkers, and standardize measurements, platforms like Altris AI transform imaging data into structured, quantifiable, and interoperable datasets. This enables pharma and clinical teams to move beyond anecdotal insights toward statistically robust, evidence-driven decision-making.
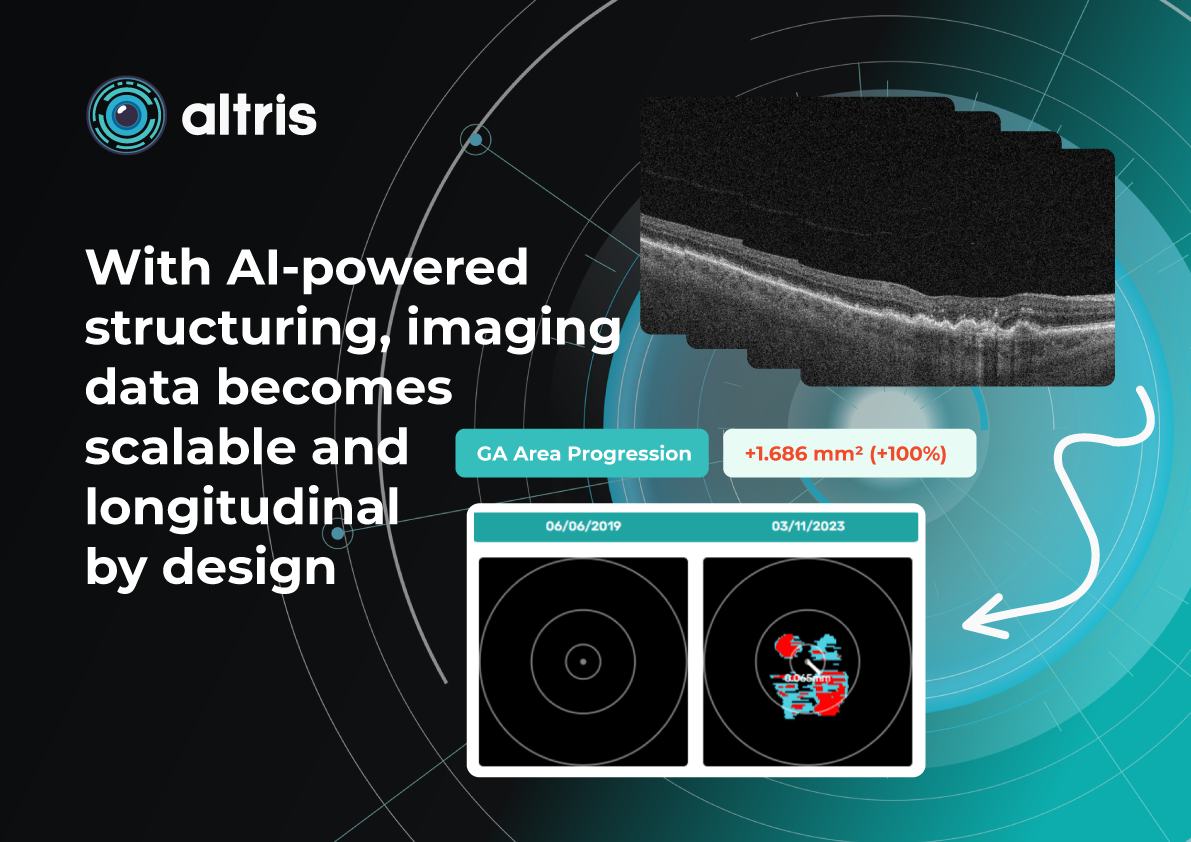
With AI-powered structuring, imaging data becomes scalable and longitudinal by design. Instead of isolated snapshots, clinicians and researchers gain continuous, comparable measurements across time, patients, and sites. This unlocks real-time monitoring of disease progression and treatment response, supports precise patient stratification, and accelerates cohort identification for therapies such as GA treatments.
Ultimately, structured imaging powered by AI bridges the gap between clinical practice and research—turning OCT into a high-value, real-time RWE engine that is both clinically meaningful and commercially actionable.
References:
https://onlinelibrary.wiley.com/doi/full/10.1111/aos.14698
https://www.visionacademy.org/media/3251/download




popular Posted
-
OCT biomarkers in diabetic macular edema: detection, quantification, and monitoring
Maria Znamenska
5 min.Table of Contents
The pathogenesis of OCT biomarkers in diabetic macular edema (DME) is complex and multifactorial. The key mechanism is disruption of the inner blood–retinal barrier resulting from chronic hyperglycemia.
- Introduction. Brief overview of diabetic macular edema (DME)
- Main OCT biomarkers of DME
2.1 Signs of DME on OCT
2.2 Quantitative parameters for monitoring DME on OCT
DME management and patient education: key aspects of the modern approach
ReferencesIntroduction. Brief Overview of Diabetic Macular Edema (DME)
The pathogenesis of OCT biomarkers in diabetic macular edema (DME) is complex and multifactorial. The key mechanism is disruption of the inner blood–retinal barrier resulting from chronic hyperglycemia. This leads to increased vascular permeability, plasma extravasation, and fluid accumulation within the retinal layers. Inflammatory processes, cytokine and growth factor activation—particularly vascular endothelial growth factor (VEGF)—also play an important role by further increasing vascular permeability and sustaining chronic edema. For this reason, DME is now regarded not only as a vascular disorder but also as a neurodegenerative and inflammatory pathology.
Morphologically, DME is characterized by retinal thickening, the formation of intraretinal cystoid spaces, accumulation of subretinal fluid, and progressive photoreceptor damage. Importantly, these structural changes often develop long before the onset of clinical symptoms. A patient may not experience significant visual deterioration, while irreversible changes are already occurring at the microstructural level. This underscores the critical importance of early diagnosis and regular monitoring.
Current clinical guidelines, including those of the American Academy of Ophthalmology, emphasize that the timely detection of DME and the early initiation of treatment significantly improve functional outcomes. However, effective patient management is impossible without precise instrumental monitoring, particularly with optical coherence tomography (OCT), which enables assessment of both the presence and progression of the pathological process.
OCT has become the imaging modality that fundamentally transformed the approach to the diagnosis and treatment of DME. It provides noninvasive visualization of the retina with micron-level resolution, allowing detailed analysis of its layered structure.
Moreover, modern tomographic systems enable a transition from qualitative to quantitative assessment. Measurement of central retinal thickness, lesion area, and other parameters provides objective monitoring of disease progression. This is especially important in the era of personalized medicine, when treatment decisions are based not only on the clinical picture but also on precise numerical indicators.
Thus, modern management of DME cannot be envisioned without the systematic use of OCT and the analysis of its biomarkers. Ophthalmology has progressed from simply detecting edema to achieving a deeper understanding of microstructural changes and their clinical significance.
The aim of this article is to summarize current evidence on OCT biomarkers of diabetic macular edema, their roles in detection, quantitative assessment, and disease monitoring, and the practical aspects of their use in clinical practice to optimize patient management.
2. Main OCT Biomarkers in DME
The modern approach to DME is based on a fundamentally new understanding of OCT’s role. OCT biomarkers in DME enable not only assessment of fluid presence but also determination of its type, localization, severity, and impact on key functional structures, particularly the photoreceptors. This is critically important because DME may have different pathogenic mechanisms across patients, ranging from vascular and inflammatory processes to a predominantly tractional component.
Particular attention should be paid to the role of OCT biomarkers in predicting the course of DME and treatment response. Features such as disorganization of the retinal inner layers (DRIL), the condition of the ellipsoid zone, and the presence of hyperreflective foci are now considered important indicators for predicting disease progression and functional outcomes. These biomarkers enable clinicians to anticipate which patients are more likely to respond favorably to anti-VEGF therapy and in which cases a less favourable visual outcome should be expected.
Each structural element observed on an OCT scan carries its own clinical significance. These findings allow the physician to answer several key clinical questions:
- how active the disease process is,
- whether the condition is acute or chronic,
- which structures have already undergone irreversible changes,
- which pathogenic mechanism predominates,
- and, most importantly, what the likely therapeutic response will be.
Thus, OCT interpretation extends far beyond simple visual assessment. It becomes an analytical process in which the clinician integrates morphological features with quantitative measurements and the patient’s clinical data.
According to current international recommendations, no single parameter—such as central retinal thickness—can be sufficient for clinical decision-making. Instead, analysis of a combination of morphological patterns, quantitative indicators, and their temporal changes is recommended.
The transition from static assessment to dynamic monitoring is particularly important via OCT biomarkers in dme. The rate of change, stability, or progression of individual biomarkers is often more informative than their absolute values. For example, a slight but persistent increase in intraretinal fluid may have greater clinical significance than a single high retinal thickness measurement.
In addition, modern technologies have considerably expanded the capabilities of OCT analysis. The use of automated retinal layer segmentation, quantitative fluid volume assessment, and artificial intelligence algorithms helps reduce subjective interpretation and improve the reproducibility of results. This is especially important both in clinical practice and in scientific research, where accuracy and standardization are essential.
In summary, the contemporary concept of OCT biomarkers in DME is based on three interconnected levels of analysis:
- Morphological level — identification of structural changes and edema type.
- Quantitative level — measurement of retinal thickness, fluid volume, and lesion area.
- Prognostic level — assessment of the risk of progression and treatment response.
It is precisely this multilevel evaluation that enables a transition from standardized treatment protocols to a personalized approach, in which the therapeutic strategy is determined by each patient’s OCT biomarker profile.
2.1 OCT Features of Diabetic Macular Edema (DME)
There are several distinct OCT patterns associated with DME, including diffuse retinal thickening, cystoid macular edema (intraretinal cystic spaces), and serous retinal detachment (subretinal fluid).
1. Diffuse retinal thickening
This is characterized by a uniform increase in macular thickness, resulting from fluid accumulation in the extracellular space of the neurosensory retina due to disruption of the inner blood–retinal barrier and an imbalance between fluid leakage and the resorptive capacity of the retinal pigment epithelium (RPE).
When cystic spaces are present, their diameter must not exceed 50 μm; otherwise, the edema is classified as cystoid.
In chronic edema (lasting more than 6–9 months), irreversible photoreceptor damage may occur, along with the development of retinal atrophy.
Key features:
- may be the only finding in early stages
- requires careful quantitative assessment (central retinal thickness, CRT measurement)
- Macular thickness dynamics are an important biomarker of treatment efficacy
2. Cystoid macular edema (intraretinal cystic spaces)
This is a key structural marker of DME. On OCT, it appears as hyporeflective, round or oval cavities, predominantly located in the inner nuclear layer (INL) and the outer plexiform layer (OPL).
Clinical significance:
- reflects vascular hyperpermeability
- indicates active edema
- large and confluent cysts may suggest a chronic process and are associated with a worse functional prognosis
Long-standing cysts can lead to mechanical stretching of retinal tissue and secondary photoreceptor damage.
3. Serous retinal detachment (subretinal fluid)
Subretinal fluid refers to the accumulation of fluid between the neurosensory retina and the retinal pigment epithelium (RPE).
On OCT, it appears as a hyporeflective space above the RPE and is associated with neurosensory retinal detachment.
Clinical interpretation:
- may be a marker of active disease
- in some cases is associated with a better response to anti-VEGF therapy
- causes less photoreceptor damage than chronic intraretinal cysts
Although subretinal fluid is generally associated with a relatively better visual prognosis, its presence requires careful monitoring and should be considered when planning anti-VEGF treatment.
2.2 Quantitative parameters for monitoring DME on OCT
After morphological assessment, the next step is quantitative analysis. Currently, several key quantitative parameters can be obtained:
- Central retinal thickness (CRT) – the most widely used parameter
- Macular volume
- Fluid quantity and volume
These measurements enable precise monitoring of treatment response and help guide decisions regarding injection intervals.
3. Management of DME and patient education: key aspects of the modern approach
Modern management of diabetic macular edema (DME) is based on a comprehensive, personalized strategy in which OCT plays a central role. Today, therapeutic decisions are influenced by the morphological type of edema, disease activity, integrity of neurosensory retinal structures, individual patient characteristics, comorbidities, and prognostic biomarkers.
A key principle of the contemporary approach is the integration of structural OCT biomarkers in DME into clinical decision-making. These biomarkers not only help determine whether treatment is necessary, but also assist in selecting the optimal therapeutic modality, assessing response, and timely adjustment of management strategy.
Additional factors influencing therapy selection include:
- Presence of disorganization of the retinal inner layers (DRIL) and disruption of the ellipsoid zone (EZ)
- Response to previous treatments
- Systemic comorbidities (renal impairment, hypertension, adherence/compliance issues)
Treatment
Anti-VEGF therapy
Anti-VEGF agents (aflibercept, ranibizumab, bevacizumab) remain the first-line treatment for DME, as they directly target the key pathogenic mechanism—vascular hyperpermeability.
Newer agents with extended durability are emerging, including implantable drug delivery systems.
However, not all patients respond equally to anti-VEGF therapy. Therefore, OCT biomarker analysis is crucial: for example, a predominance of intraretinal cystic changes is usually associated with a good response to anti-VEGF, whereas a high number of hyperreflective foci or signs of chronic edema may indicate a significant inflammatory component and support consideration of steroid therapy.
Intravitreal corticosteroid implants
Steroids are used in cases of chronic and refractory DME, insufficient response to anti-VEGF therapy, and in patients with a pro-inflammatory phenotype.
Laser therapy
Although laser treatment has become less central in current practice, it remains useful in selected clinical scenarios. Subthreshold micropulse laser is more commonly used in patients with focal edema without involvement of the foveal center.
Thus, treatment decisions today are no longer universal; they are based on an individualized OCT-based patient profile.
Role of OCT in treatment
OCT accompanies the patient throughout all stages of treatment and performs several key functions:
- determination of indications for initiating therapy (presence of fluid, macular thickening, involvement of the foveal region)
- assessment of treatment response (reduction of fluid, normalization of thickness, structural restoration)
- detection of resistance or partial response
- optimization of injection intervals (treat-and-extend or pro re nata strategies)
A particularly important aspect is that OCT can detect subclinical changes. For example, minimal fluid accumulation may appear before any subjective deterioration in vision. This enables timely treatment adjustments and the prevention of functional loss.
In addition, OCT helps avoid both under- and overtreatment. In patients with a stable anatomical profile and no fluid, injection intervals can be gradually extended, reducing the burden on both the patient and the healthcare system.
Monitoring
The frequency of follow-up depends on disease stage and activity:
- active treatment phase – monthly visits with OCT control
- stabilization phase – every 2–4 months
- long-term follow-up – individualized, depending on recurrence risk and associated risk factors
It is important to emphasize that monitoring must remain regular even in the absence of symptoms. DME can progress asymptomatically, and only OCT allows objective assessment of retinal status.
Dynamic follow-up is critical: comparison of sequential scans provides the most valuable information about disease progression.
What is important to explain to the patient
Effective management of DME is not possible without active patient participation; therefore, communication is a key component of treatment.
The patient must clearly understand that:
- DME is a chronic condition requiring long-term monitoring
- treatment aims to stabilize and slow disease progression, not always to fully restore vision
- interruption of therapy without medical advice may lead to deterioration
- regular visits and OCT monitoring are critical, even if vision appears stable
It is especially important to explain the role of OCT to patients. Showing scans and explaining changes significantly improves treatment adherence.
Lifestyle and systemic control
Since diabetic macular edema (DME) is a complication of a systemic disease, control of the patient’s overall health is of critical importance.
Key recommendations include:
- optimal glycemic control
- blood pressure management
- correction of lipid profile
- healthy diet rich in antioxidants
- regular physical activity
- smoking cessation
Psychological aspects and treatment adherence
DME often follows a long and fluctuating course, which may lead to treatment fatigue or reduced motivation in patients. Many patients underestimate the severity of the condition, especially in early stages when visual acuity is still preserved.
In this context, OCT becomes not only a diagnostic tool but also a communication instrument. Visualization of pathological changes helps patients better understand the disease and the necessity of treatment.
Establishing a partnership between physician and patient is essential for successful long-term management.
Conclusion
OCT biomarkers in DME now allow not only precise diagnosis but also an approach that goes far beyond traditional retinal assessment. Thanks to its high resolution and ability to visualize microstructural changes, OCT enables the detection of subtle abnormalities before clinically significant symptoms appear. This opens the way to a new level of patient management—shifting from descriptive assessment to quantitative evaluation of pathological changes, their dynamics, and treatment response. Furthermore, OCT biomarker analysis allows prediction of disease course, identification of progression risk, and individualization of therapeutic strategies for each patient.
Modern DME management is not just diagnosis and treatment, but a comprehensive clinical decision-making system based on objective, standardized data. There is a clear shift from subjective interpretation of fundus changes to structured analytics, where every parameter matters: retinal thickness, presence of intra- or subretinal fluid, status of outer retinal layers, and macular architectural disruption. OCT has become the key tool transforming clinical practice, making it more precise, reproducible, and evidence-based. It allows clinicians not only to confirm the presence of pathology but also to better understand its nature, activity, and potential reversibility.
Ultimately, effective DME management today is the result of synergy between modern imaging technologies, clinical reasoning, and active patient engagement. Proper interpretation of OCT images must be integrated into the overall clinical picture, taking into account systemic factors, diabetes duration, and individual patient characteristics. In this process, OCT acts as a central link—a bridge between diagnosis and treatment—uniting all oct biomarkers in diabetic macular edema components into a coherent clinical system. This approach leads to better functional outcomes, preservation of vision, and significant long-term improvement in patients’ quality of life.
FAQ
1. How can AI help detect OCT biomarkers in DME?
AI can automatically identify key OCT biomarkers such as intraretinal fluid, subretinal fluid, hyperreflective foci, and retinal layer disruptions, helping clinicians detect disease activity faster and more consistently.
2. Why is quantitative biomarker analysis important in DME?
Quantification enables objective measurement of biomarker volume, area, and progression over time, supporting treatment decisions, therapy response assessment, and longitudinal patient monitoring.
3. Which OCT biomarkers are most relevant for monitoring DME progression?
Commonly monitored biomarkers include intraretinal fluid (IRF), subretinal fluid (SRF), hyperreflective foci (HRF), disorganization of retinal inner layers (DRIL), and ellipsoid zone disruption.
4. How can automated OCT analysis improve clinical workflow?
Automated analysis reduces manual interpretation time, improves reproducibility, standardizes reporting, and helps clinicians prioritize patients who may require closer follow-up or treatment adjustments.
References
- https://pubmed.ncbi.nlm.nih.gov/38460657/
- https://brief.euretina.org/research/association-of-retinal-oct-biomarkers-with-reading-performance-in-patients-with-diabetic-macular-edema-dme
- https://www.mdpi.com/2075-4418/14/1/76
- https://www.sciencedirect.com/science/article/pii/S1572100024000814
- https://link.springer.com/article/10.1186/s40942-023-00473-w
- https://www.medscape.com/viewarticle/1001580
- https://www.cureus.com/articles/227801-innovations-in-diabetic-macular-edema-management-a-comprehensive-review-of-automated-quantification-and-anti-vascular-endothelial-growth-factor-intervention#!/
-
RWE in Ophthalmology: Challenges of Collection and Processing
Maria Znamenska
3 min.Pharma has no shortage of data in ophthalmology—EHRs, imaging repositories, claims, registries—but the industry still faces a persistent RWE gap when it comes to turning that data into commercially actionable insight.
This gap becomes especially critical in the context of modern ophthalmic therapies, where timing, disease stage, and adherence directly impact outcomes—and, by extension, market performance. Without precise, scalable ways to identify eligible patients (e.g., early-stage AMD, DME with specific biomarkers), commercial teams are left relying on proxies or delayed claims data. At the same time, tracking real-world outcomes remains reactive and retrospective, limiting the ability to support value-based narratives, optimize field strategy, or respond dynamically to physician behavior.
For commercial and market access leaders, closing the RWE gap is no longer a “data strategy” initiative—it’s a growth imperative. The organizations that will lead are those that move beyond passive data aggregation toward active, AI-driven interpretation of multimodal ophthalmic data, enabling near real-time patient identification and outcome tracking. This shift not only strengthens evidence generation but directly translates into sharper targeting, more credible value communication, and ultimately, stronger adoption curves in an increasingly competitive therapeutic landscape.
RWE Key Components
Real-world evidence (RWE) in ophthalmology is fundamentally multimodal—it emerges from the combination of
- OCT imaging,
- clinical metrics,
- treatment patterns,
- and patient context over time.
When these components are connected, they move beyond descriptive data and become decision-grade insight for commercial, medical, and market access teams.
Imaging (OCT): the gold mine of RWE
OCT is the anchor, but only when integrated with outcomes, treatment data, and longitudinal context does it unlock its full commercial value—turning raw data into actionable RWE that can directly shape strategy and growth.
Leverage data from past or ongoing clinical trials with the ability to standardize it within a unified ecosystem. OCT segmentation model can enable you to extract robust, clinically meaningful insights from your trial data to:
- Gain a deeper understanding of patient responses to treatments by characterizing disease progression and outcomes over time.
- Segment patient populations into subgroups to evaluate biomarker-driven profiles and build predictive analytics—helping streamline future trials by refining endpoints and optimizing inclusion and exclusion criteria.
All that, as well as to build one of the most extensive and comprehensive real-world evidence (RWE) databases in ophthalmology may be quite possible within one OCT-vendor neutral data analysis platform ecosystem.
Clinical outcomes: functional reality
Clinical measures—most notably visual acuity (VA), intraocular pressure, and physician-reported assessments—represent the functional impact of disease and treatment. These endpoints are still central to regulatory and commercial narratives, but in isolation they are often lagging indicators. By the time vision declines, disease progression may already be advanced. When paired with imaging, however, clinical outcomes provide the critical link between anatomical change and patient benefit, strengthening real-world value stories and payer communication.
RWE delivers critical insights into how therapies perform in routine clinical practice—such as healthcare outcomes, treatment adherence, and protocol efficiency—often revealing patterns that differ from those observed in controlled clinical trials.
Treatment data: what actually happens in practice
Treatment data captures real-world behavior—which therapies are used, dosing frequency, switching patterns, and adherence. This is where the gap between clinical trial protocols and actual practice becomes visible. For commercial teams, this layer reveals drop-off points, under-treatment, and competitive dynamics at a granular level. When combined with OCT and outcomes, this approach makes it possible to understand not just what is happening but why—for example, whether discontinuation is driven by lack of response, disease stabilization, or operational constraints.
OCT segmentation enables high-throughput processing and deep interrogation of large-scale datasets, enhancing the interpretation of real-world data. It can validate existing assumptions, uncover new patterns, and support hypothesis generation and testing. This analysis provides a clearer view of treatment efficacy and safety, disease progression in real-world settings, and a more precise understanding of target patient populations.
Demographics and patient context
Demographics (age, gender, geography) and broader patient context (comorbidities, access to care) provide the segmentation layer for RWE. These factors influence disease prevalence, treatment eligibility, and adherence patterns. While less granular than imaging, they are essential for market sizing, targeting, and equity considerations, helping commercial leaders understand where the highest-value opportunities—and barriers—exist across populations.
Data analysis includes population-level distributions of retinal layer thickness and fluid volumes; longitudinal tracking of layer and fluid changes over time; and assessment of retinal layer attenuation/loss (depletion maps) and atrophic regions (Figure 2), among other endpoints.
Longitudinal progression: the real differentiator
The true power of RWE lies in its longitudinal nature—tracking how patients evolve over time across imaging, outcomes, and treatment. This enables identification of disease trajectories, early signals of response or non-response, and optimal intervention windows. For pharma decision-makers, longitudinal RWE transforms static snapshots into predictive insight, supporting earlier intervention strategies, more precise patient journeys, and stronger, evidence-backed differentiation in crowded markets.
The Core Problem
There are core RWE problems worth mentioning. pay attention to the following bottlenecks: fragmented data, unstructured imaging, lack of standardization, and broken longitudinal tracking.
- Fragmented data: Patient information is dispersed across multiple systems, limiting the ability to generate a unified, comprehensive view.
- Unstructured imaging: Large volumes of imaging data, such as OCT scans, remain unstructured and difficult to analyze at scale.
- Lack of standardization: Variability in data formats and clinical protocols hinders consistent analysis and comparison.
- Broken longitudinal tracking: Incomplete or disconnected patient timelines prevent accurate assessment of disease progression and treatment outcomes over time.
The core issue isn’t volume; it’s fragmentation and lack of standardization. OCT scans sit in one system, visual acuity in another, treatment histories elsewhere, often unstructured or inconsistently coded. As a result, even well-resourced teams struggle to answer seemingly simple questions like: Who are the untreated but eligible patients? or Which cohorts are actually benefiting from therapy in real-world settings?
However, AI is transforming the RWE in ophthalmology research to:
- Design smarter, biomarker-driven trials
- Estimate disease burden and patient volumes
- Track outcomes, safety, and progression
- Strengthen regulatory and market access strategies
Resources to aid ophthalmologists in evaluating the quality of RWE are available, such as the Good Research for Comparative Effectiveness (GRACE) principles, which can support the evaluation of observational comparative effectiveness studies.
GRACE checklist to support ophthalmologists in the evaluation of RWE:
Data Methods ✓ Were treatment and/or important details of treatment exposure adequately recorded for the study purpose in the data source(s)? ✓ Was the study (or analysis) population restricted to new initiators of treatment or those starting a new course of treatment? ✓ Were the primary outcomes adequately recorded for the study purpose? ✓ If one or more comparison groups were used, were they concurrent comparators? If not, did the authors justify the use of historical comparison groups? ✓ Was the primary clinical outcome(s) measured objectively rather than subject to clinical judgment? ✓ Were important confounding and effect-modifying variables taken into account in the design and/or analysis? ✓ Were primary outcomes validated, adjudicated, or otherwise known to be valid in a similar population? ✓ Is the classification of exposed and unexposed person-time free of “immortal time bias”? ✓ Was the primary outcome(s) measured or identified in an equivalent manner between the treatment/intervention group and the comparison group? ✓ Were any meaningful analyses conducted to test key assumptions on which primary results are based? ✓ Were important covariates that may be known confounders or effect modifiers available and recorded? *Table adapted from Dreyer NA et al. J Manag Care Pharm 2014; 20 (3): 301–308 (Table 1). While used with permission of the publisher, the publisher disclaims all endorsement of any organization, product or technique as a matter of policy.
Why Imaging Is Critical?
OCT is a stepping stone to understanding Geographic Atrophy. Since the approval of the first therapy targeting geographic atrophy in early 2023, interest in the disease has increased dramatically. At the same time, a growing number of clinical trials are underway, evaluating the safety and efficacy of multiple investigational compounds.
Imaging—particularly OCT (optical coherence tomography)—is the backbone of meaningful real-world evidence in retinal disease, because it captures what clinical codes and claims data simply cannot: anatomical change over time. Without structured OCT data, RWE becomes fragmented and largely inferential, relying on indirect proxies like treatment patterns or visual acuity alone. This creates a major blind spot in understanding disease progression, especially in chronic degenerative conditions where structural deterioration often precedes functional loss.
In geographic atrophy (GA), this gap is especially critical for therapies such as Syfovre (pegcetacoplan) and Izervay (avacincaptad pegol). These treatments are designed to slow structural progression, not just improve symptoms, meaning their real-world impact can only be properly assessed through consistent, longitudinal imaging markers—lesion growth, retinal layer integrity, and atrophy expansion. When OCT data is unstructured or missing, it becomes impossible to reliably track these anatomical endpoints across time and across care settings.
As a result, RWE datasets without standardized OCT integration fail to support robust patient journey reconstruction, dilute treatment effect signals, and limit the ability to identify responders vs non-responders. For pharma and clinical stakeholders, this means missed opportunities to demonstrate value, optimize patient selection, and build predictive models that depend on continuous structural imaging rather than episodic clinical snapshots.
The Way Forward
AI-driven structuring of imaging data is emerging as the missing link between raw clinical information and truly actionable real-world evidence (RWE). In ophthalmology, vast volumes of OCT scans remain underutilized because they are stored as unstructured images, making large-scale analysis slow, inconsistent, and often impractical.
By applying advanced algorithms to automatically segment retinal layers, detect biomarkers, and standardize measurements, platforms like Altris AI transform imaging data into structured, quantifiable, and interoperable datasets. This enables pharma and clinical teams to move beyond anecdotal insights toward statistically robust, evidence-driven decision-making.
With AI-powered structuring, imaging data becomes scalable and longitudinal by design. Instead of isolated snapshots, clinicians and researchers gain continuous, comparable measurements across time, patients, and sites. This unlocks real-time monitoring of disease progression and treatment response, supports precise patient stratification, and accelerates cohort identification for therapies such as GA treatments.
Ultimately, structured imaging powered by AI bridges the gap between clinical practice and research—turning OCT into a high-value, real-time RWE engine that is both clinically meaningful and commercially actionable.
References:
https://onlinelibrary.wiley.com/doi/full/10.1111/aos.14698
https://www.visionacademy.org/media/3251/download
-
PBM Monitoring on OCT: Drusen Progression
Maria Znamenska
5 min.Introduction: Role of PBM in Retinal Disease Management
Photobiomodulation (PBM), also referred to as low-level light or laser therapy, has emerged as a promising non-invasive therapeutic strategy in ophthalmology, particularly for the management of retinal diseases. PBM utilizes low-energy light in the red-to-near-infrared spectrum (typically 600–1000 nm) to modulate cellular function through photochemical rather than thermal mechanisms.
According to Retina Today, PBM is being used as an adjunctive or alternative treatment for several retinal diseases, including age-related macular degeneration (AMD), diabetic retinopathy (DR), and diabetic macular edema (DME). Its advantages include a favorable safety profile, non-invasive delivery, and relatively low cost compared to conventional therapies. Furthermore, advances in light-emitting diode (LED) technology have facilitated broader clinical application by enabling safe, uniform, and cost-effective retinal illumination.
Key OCT Biomarkers to Track During PBM Therapy
Optical coherence tomography (OCT) has become an indispensable tool for monitoring retinal structure and treatment response in patients undergoing photobiomodulation (PBM) therapy. Given the mechanism of PBM—targeting mitochondrial function, reducing oxidative stress, and modulating inflammation—several OCT-derived biomarkers are particularly relevant for assessing therapeutic efficacy of dry AMD progression and in other retinal disorders.
In this article, I will show how to quantify and monitor OCT biomarkers for effective PBM monitoring.
1. PBM monitoring on OCT: Drusen Progression
For patients on photobiomodulation (PBM), OCT monitoring of drusen is about one core question: Are we stabilizing or reversing RPE–Bruch’s membrane dysfunction, or is the eye still progressing toward atrophy? So, on B-scans, drusen are seen as:
- RPE elevations (dome-shaped or irregular)
- Material between RPE and Bruch’s membrane
- Variable internal reflectivity
Here are the key drusen biomarkers to track under PBM:
- Drusen volume (MOST important)
- Measured via OCT segmentation (cube scans)
- It represents the total disease burden
As the PBM goal here is the stabilisation or reduction in drusen volume
Red flag:
- Continuous increase → disease progression
- Drusen height & area
- Local structural impact on photoreceptors
PBM signal:
- Flattening = potential response
- Increasing height = worsening RPE dysfunction
- Internal reflectivity
- Homogeneous vs heterogeneous content
An important nuance is that increasing heterogeneity may indicate:
- calcification
- regression OR collapse before atrophy
So, it needs to be correlated with other signs.
You may observe Drusen regression patterns. However, not all regression is good.

“Good” regression:
- Gradual flattening
- No photoreceptor loss
- Stable RPE
“Bad” regression (collapse):
- Sudden disappearance
- Followed by:
- RPE loss
- outer retinal thinning
Leads to geographic atrophy (GA)
To summarise, for PBM-treated patients, prioritize:
- Drusen volume trend (longitudinal)
- Photoreceptor integrity (EZ/ONL)
- Signs of atrophy risk (HRF, collapse patterns)
Dry AMD progression matters in PBM monitoring. PBM is currently aimed at:
- early → intermediate dry AMD
So when you monitor drusen on OCT, you’re not just tracking morphology — you’re tracking disease trajectory: Is the eye staying in intermediate AMD, or moving toward advanced stages (GA / nAMD)?
2. Central retinal thickness (CRT)
In addition to PBM monitoring on OCT: Drusen progression, one of the primary biomarkers is also central retinal thickness (CRT), which reflects changes in retinal edema and overall retinal integrity. Reductions in CRT during PBM therapy may indicate decreased inflammatory activity and improved fluid homeostasis, particularly in conditions such as diabetic macular edema (DME) and neovascular retinal diseases. However, in non-exudative conditions such as dry age-related macular degeneration (AMD), CRT changes may be subtle, necessitating the evaluation of additional structural parameters.
3. The outer retinal layers
The outer retinal layers, especially the integrity of the ellipsoid zone (EZ) and external limiting membrane (ELM), represent critical biomarkers of photoreceptor health. PBM has been associated with improved mitochondrial activity within photoreceptors, and preservation or restoration of EZ continuity on OCT may serve as a surrogate marker of functional recovery. Disruptions in these layers are strongly correlated with visual impairment, making them highly relevant endpoints in PBM studies.
4. Retinal pigment epithelium (RPE)
Another key biomarker is retinal pigment epithelium (RPE) morphology, including the presence and evolution of drusen, subretinal drusenoid deposits (SDD), and RPE irregularities. PBM has been hypothesized to enhance RPE function and reduce oxidative burden, potentially leading to stabilization or regression of drusen volume over time. Quantitative drusen analysis using OCT can therefore provide insight into disease modification, particularly in intermediate AMD.
5. Hyperreflective foci (HRF)
Hyperreflective foci (HRF) are also important indicators of retinal inflammation and microglial activation. A reduction in HRF number or density during PBM therapy may reflect decreased inflammatory signaling, aligning with the known anti-inflammatory effects of light-based treatment. Similarly, subretinal and intraretinal fluid—when present—should be carefully monitored, as their resolution may indicate improved retinal barrier function and treatment response.
PBM Treatment Monitoring Protocol
1. Patient Selection and Baseline Assessment
Appropriate patient selection is crucial for optimizing the outcomes of photobiomodulation (PBM) therapy in the progression of dry AMD. Current evidence supports its use primarily in non-exudative retinal diseases, particularly intermediate Age-related Macular Degeneration, as well as emerging applications in Diabetic Retinopathy and Diabetic Macular Edema.
Inclusion considerations:
- Intermediate AMD (presence of drusen and/or subretinal drusenoid deposits)
- Stable retinal conditions without active neovascularization
- Best-corrected visual acuity (BCVA) is sufficient for functional monitoring
Exclusion criteria:
- Active neovascular AMD or significant intraretinal/subretinal fluid
- Recent anti-VEGF injections (unless PBM is used adjunctively in controlled settings)
- Significant media opacity affecting light delivery or imaging quality

Baseline evaluation should include:
- Visual function testing: BCVA, contrast sensitivity
- Structural imaging: spectral-domain OCT (mandatory)
- Optional advanced imaging: OCT angiography (OCTA) for vascular assessment
- Key OCT biomarkers (baseline reference):
- Central retinal thickness (CRT)
- Ellipsoid zone (EZ) integrity
- Retinal pigment epithelium (RPE) status and drusen volume
- Presence of hyperreflective foci (HRF)
Establishing a robust baseline is essential, as PBM-induced changes are often gradual and require longitudinal comparison.
2. Treatment Session Procedure
PBM is delivered using low-level light in the red-to-near-infrared spectrum (typically ~600–1000 nm), most commonly via LED-based systems designed for retinal applications.
Standard session workflow:
- Patient preparation
- No pharmacologic dilation is typically required (device-dependent)
- Proper alignment and fixation ensured
- Device application
- Light delivered trans-pupillary using controlled, non-thermal energy
- Multi-wavelength protocols (e.g., combinations of ~590 nm, 660 nm, 850 nm) are commonly used in clinical studies
- Treatment duration
- Typically, a few minutes per eye per session (device-specific)
- Sequential or simultaneous bilateral treatment, depending on the system
- Safety monitoring
- PBM is non-invasive and well-tolerated
- No significant adverse retinal effects have been reported in the current literature
- Monitor for discomfort or visual disturbances
- Immediate post-session:
- No recovery time required
- Patients resume normal activities immediately
The mechanism of action—enhancing mitochondrial activity and reducing oxidative stress—does not produce immediate anatomical changes, reinforcing the need for structured follow-up.
3. Treatment Series and Frequency
PBM is not a single-session therapy for observing dry AMD progression or any other condition, but is administered as a treatment series, followed by monitoring and potential retreatment cycles.
Typical treatment regimen (based on clinical studies):
- Induction phase:
- 2–3 sessions per week
- Duration: 3–5 weeks
- Total: ~9–12 sessions per cycle
- Follow-up period:
- Reassessment at 1–3 months post-treatment
- OCT imaging to evaluate structural response
- Retreatment strategy:
- Repeat cycles every 4–6 months, depending on disease progression and response
- Individualized based on OCT biomarkers and functional outcomes
Monitoring during and after therapy:
- Short-term (during treatment):
- Limited structural change expected
- Intermediate-term (1–3 months):
- Possible reduction in drusen volume
- Stabilization of EZ and RPE integrity
- Decrease in HRF (inflammatory markers)
- Long-term:
- Disease stabilization rather than reversal is the primary goal
Outcome measures:
- Functional: BCVA, contrast sensitivity
- Structural: OCT biomarkers (drusen, EZ, CRT, HRF)
- Optional: OCTA vascular parameters
A structured PBM protocol integrates careful patient selection, standardized treatment delivery, and longitudinal OCT-based monitoring. The therapy is best suited for chronic, non-exudative retinal conditions, where its cumulative biological effects—rather than immediate anatomical changes—drive clinical benefit. Consistent imaging and biomarker tracking are essential for guiding retreatment decisions and evaluating long-term efficacy.
Clinical Application and Results
The integration of digital technologies and artificial intelligence (AI) into retinal imaging has significantly enhanced the ability to monitor treatment response in photobiomodulation (PBM) therapy. Given that PBM induces gradual, often subtle structural and functional changes, advanced analytical tools are essential for detecting and quantifying these effects with precision and reproducibility. Here are some real cases of application in Ophthalmology (Dry AMD, DME, etc).
Dry AMD case
Photobiomodulation (PBM) has been clinically evaluated primarily in patients with early-to-intermediate Age-related Macular Degeneration, where no widely accepted disease-modifying therapy exists. The most robust evidence comes from the LIGHTSITE clinical trial program, in which PBM is delivered as multiwavelength light therapy (590, 660, and 850 nm) in repeated treatment cycles (typically 9 sessions over 3–5 weeks, repeated every 4 months).
Across the LIGHTSITE I–III studies, PBM has consistently demonstrated functional improvements, particularly in best-corrected visual acuity (BCVA) and contrast sensitivity, and has shown favorable safety outcomes, with no evidence of phototoxicity. In LIGHTSITE II, PBM-treated eyes showed a mean ~4-letter gain in BCVA at 9 months, with approximately one-third of patients achieving ≥5-letter improvement, while sham-treated eyes showed minimal change. Earlier studies also reported improvements in contrast sensitivity, microperimetry, and reductions in drusen burden, suggesting both functional and anatomical benefits .
More recent data from the pivotal LIGHTSITE III trial further support these findings, demonstrating statistically significant gains in visual acuity compared with sham treatment, with mean improvements exceeding 5 letters and a substantial proportion of patients achieving clinically meaningful gains. At 24 months, PBM-treated eyes showed sustained visual improvement (+6.2 letters) and a reduced progression to geographic atrophy (6.8% vs 24.0% in controls), suggesting potential disease-modifying effects.
However, despite these encouraging results, meta-analyses indicate that overall effect sizes remain modest and that variability across studies, small sample sizes, and protocol heterogeneity limit definitive conclusions regarding long-term clinical benefit. Thus, while PBM represents a promising and biologically plausible therapy for dry AMD, its role in routine clinical practice continues to evolve, with ongoing studies needed to confirm durability, optimal patient selection, and real-world effectiveness.
DME
Photobiomodulation (PBM) has been explored as a non-invasive adjunctive or alternative therapy for Diabetic Macular Edema, targeting key pathogenic mechanisms, including mitochondrial dysfunction, oxidative stress, and chronic inflammation.
Unlike anti-VEGF therapy, which primarily addresses vascular permeability, PBM aims to restore retinal metabolic balance through light-induced activation of mitochondrial pathways. Early clinical studies using red-to-near-infrared wavelengths (typically ~630–850 nm) have demonstrated reductions in central retinal thickness (CRT) and improvements in retinal morphology on OCT, alongside stabilization or modest gains in best-corrected visual acuity (BCVA). These effects are particularly notable in mild-to-moderate DME and in patients with non-center-involving edema, where PBM may reduce inflammatory signaling and improve fluid homeostasis.
Clinical data, although still limited compared to age-related macular degeneration, suggest that PBM may have value as an adjunct to standard of care, potentially reducing treatment burden in patients requiring repeated intravitreal injections. Some studies report decreased intraretinal fluid and improvement in OCT biomarkers following PBM treatment cycles, with a favorable safety profile and no evidence of retinal damage.
However, results remain heterogeneous, with variability in treatment protocols, patient populations, and outcome measures. Importantly, PBM has not yet demonstrated efficacy comparable to anti-VEGF therapy in center-involving DME, and its role is best considered complementary rather than substitutive at this stage. Larger randomized controlled trials are needed to define optimal dosing strategies, identify responder phenotypes, and clarify long-term functional benefits in DME management.
Why is OCT Critical for PBM Monitoring?
Optical Coherence Tomography (OCT) is essential for monitoring photobiomodulation (PBM) therapy because PBM aims to induce subtle, progressive structural and functional changes in the retina—especially in conditions like dry AMD progression.
Unlike anti-VEGF treatments, where effects can be more immediate, PBM outcomes are gradual and microstructural, such as changes in drusen volume, RPE integrity, outer retinal layers, and choriocapillaris perfusion. These changes are often invisible on fundus photography or visual acuity alone, making OCT the only practical tool for objective, layer-by-layer tracking over time.
Serial OCT scans allow clinicians to detect early signals of response (e.g., drusen regression or stabilization) and differentiate them from natural disease progression, which is critical for validating PBM efficacy in real-world practice.
AI-Assisted OCT Analysis
Artificial intelligence–driven analysis of optical coherence tomography (OCT) enables automated, quantitative assessment of retinal biomarkers critical to PBM monitoring. Machine learning and deep learning algorithms can segment retinal layers and identify pathological features such as drusen, hyperreflective foci (HRF), and fluid compartments with high accuracy.
In the context of PBM, AI tools provide:
- Automated retinal layer segmentation, including ellipsoid zone (EZ) and retinal pigment epithelium (RPE)
- Quantification of drusen volume and distribution, particularly relevant in Age-related Macular Degeneration
- Detection and tracking of subtle structural changes over time that may not be apparent on qualitative review
These capabilities are especially important because PBM effects are often incremental rather than dramatic, requiring sensitive longitudinal comparison.
Longitudinal Tracking and Progression Analysis
Digital platforms enable time-series analysis of OCT data, allowing clinicians to monitor the disease trajectory before, during, and after PBM therapy. Automated registration of sequential scans ensures that the same retinal locations are compared over time.
Key advantages include:
- Change detection algorithms for early identification of treatment response
- Trend analysis of biomarkers such as central retinal thickness, EZ integrity, and HRF density
- Objective progression metrics, reducing inter-observer variability
Such tools are critical for distinguishing true therapeutic effects from natural fluctuations in disease, particularly in slowly progressing conditions like dry AMD progression.
Digital tools and AI are transforming PBM monitoring by enabling precise, quantitative, and longitudinal assessment of retinal biomarkers. From automated OCT analysis to AI-driven decision support and remote monitoring, these technologies address the key challenge of PBM therapy—detecting subtle, progressive changes over time, like in dry AMD progression, etc. Their continued development will be essential for standardizing PBM protocols and optimizing patient outcomes in retinal disease management.
Altris for PBM monitoring on OCT: Drusen Progression +40 biomarkers for Research Purposes
Altris has contributed to PBM monitoring on OCT: Drusen progression, as well as 40+ other biomarkers and 30+ pathologies, which may be monitored with the system. Altris enhances this process by turning OCT into a quantitative, standardized monitoring system rather than a subjective review. It automatically segments retinal layers and biomarkers (e.g., drusen, hyperreflective foci, fluid), calculates precise volumetric metrics, and enables longitudinal comparison across visits with high reproducibility.
How does Altris assist with the monitoring of the main biomarkers of PBM therapy?
Drusen
Detection: ✔️
Quantification: ✔️ (area, volume, thickness)
Tracking over time: ✔️
This is one of the strongest use cases, which is critical for effective PBM monitoring.
Central Retinal Thickness (CRT)
Detection: ✔️
Standard ETDRS maps: ✔️
Longitudinal tracking: ✔️
Outer retinal layers (EZ, ONL, etc.)
Segmentation: ✔️ (layer-based)
Quantification: ✔️ (thickness, integrity)
Disruption detection: ✔️
This is very important for PBM response and detection of early functional damage.
RPE (Retinal Pigment Epithelium)
Detection (layer): ✔️
Elevation (drusen): ✔️
Atrophy signs: ✔️ (via hypertransmission, thinning)
Important for: drusen interpretation and GA risk, though, not always a standalone numeric biomarker.
Hyperreflective foci (HRF)
Detection: ✔️
Localization: ✔️
Counting / burden tracking: ✔️
These are high-value biomarkers for progression risk in PBM monitoring.
Assistance like this allows clinicians to track PBM response objectively, identify responders vs non-responders earlier, and generate consistent reports for clinical decision-making or research. In short, while OCT provides the necessary imaging depth, Altris unlocks its full value for PBM by making subtle retinal changes measurable, comparable, and clinically actionable.
Conclusion
PBM represents a novel and biologically plausible therapeutic modality that targets key pathological mechanisms in retinal disease. By enhancing mitochondrial function, reducing oxidative stress, and modulating inflammation, PBM holds significant potential to complement existing treatment strategies and improve outcomes in retinal disease management. However, further research is required to fully define its role in routine clinical practice.
Despite the promising findings, the clinical integration of PBM remains in an evolving stage. Variability in treatment parameters—including wavelength, dose, and treatment protocols—has limited standardization and comparability across studies. Moreover, much of the current evidence is derived from small-scale clinical trials and preclinical models, underscoring the need for large, randomized controlled trials to establish optimal treatment regimens for dry AMD progression and to assess long-term efficacy in other eye pathologies.
In this context, OCT—especially when enhanced with AI-driven analysis—plays a critical role in advancing PBM adoption. Quantitative OCT biomarkers such as drusen volume, outer retinal integrity, and subtle structural changes provide objective endpoints for assessing therapeutic response. AI-based platforms further enable precise, reproducible, and longitudinal analysis of these changes, helping to standardize evaluation, identify responders earlier, and strengthen the clinical evidence base for PBM.
FAQ Section
1. How do I objectively measure response to PBM therapy?
Clinicians look for quantifiable OCT biomarkers, not just visual acuity:
- Drusen volume (regression or stabilization)
- Outer retinal layer integrity (EZ, RPE)
- Hypertransmission / atrophy areas
The challenge: changes are subtle → require precise, longitudinal OCT comparison.
2. Which OCT biomarkers are most relevant for PBM monitoring?
The most discussed and clinically relevant:
- Drusen volume/area
- RPE atrophy
- Hypertransmission
- Ellipsoid Zone (EZ) disruption/loss
- Hyperreflective foci (secondary)
For GA specifically:
Overlap of RPE atrophy + hypertransmission + EZ loss = key composite metric.
3. How often should I monitor patients on PBM?
Typical real-world patterns:
- Baseline OCT before starting PBM
- Follow up every 3–6 months
- More frequent (monthly) in studies.
4. How do I distinguish PBM effect from natural AMD progression?
Distinguishing the effect of PBM from the natural progression of AMD remains one of the key clinical challenges. AMD typically progresses slowly and can show natural fluctuations, while PBM-related changes tend to be gradual and relatively modest. To differentiate between the two, clinicians rely on consistent OCT metrics tracked over time, comparing trends rather than single visits. Bilateral analysis—evaluating treated versus untreated eyes—can provide additional context, while assessing the rate of change, such as slowing of drusen growth or stabilization of atrophic areas, helps determine whether observed changes are likely treatment-related rather than part of the disease’s natural course.
5. Do I need AI/software for PBM monitoring, or is manual OCT review enough?
Whether AI/software is needed for PBM monitoring versus manual OCT review is an increasingly important question in clinical practice. While manual assessment can provide a general, qualitative understanding, it is often variable, time-consuming, and limited in its ability to detect subtle changes. PBM, however, requires identification of micron-level structural differences and high reproducibility across visits to accurately assess treatment response. AI-based OCT analysis addresses these challenges by enabling automated segmentation of key biomarkers, delivering precise volumetric measurements, and supporting reliable longitudinal tracking in standardized units such as mm², mm³, and percentage change. This level of consistency also helps clinicians more confidently distinguish responders from non-responders, making monitoring more objective and clinically actionable.
References:
https://pmc.ncbi.nlm.nih.gov/articles/PMC11488463/
https://link.springer.com/article/10.1007/s40135-025-00340-x
https://d-nb.info/136218389X/34
https://www.frontiersin.org/journals/ophthalmology/articles/10.3389/fopht.2024.1388602/full
https://retinatoday.com/articles/2020-may-june/photobiomodulation-as-a-treatment-in-dry-amd
https://espansionegroup.it/it/
-
Geographic Atrophy Retina OCT Biomarkers: Detection, Quantification, and Monitoring
Maria Znamenska
5 min.Introduction. Overview of Geographic Atrophy (GA) as a Late Stage of Dry AMD
Geographic atrophy (GA) is a chronic progressive retinal degeneration that represents part of the late stage of age-related macular degeneration (AMD). It is characterized by gradual and irreversible atrophy of photoreceptors, the retinal pigment epithelium (RPE), and the choriocapillaris. As a result, a persistent defect of neurosensory tissue develops, which clinically manifests as central vision loss, the appearance of central scotomas, and reduced contrast sensitivity.
Atrophic lesions typically originate in the outer retinal layers and gradually expand, involving the macula and fovea. Over time, this leads to irreversible visual impairment and a significant decline in quality of life. In the early stages, patients may not experience noticeable changes in visual acuity. However, involvement of the central foveal region may lead to a sudden functional deterioration, with patients reporting difficulties in reading, recognizing faces, and working with fine details.
GA is considered one of the leading causes of clinically significant central blindness among people over the age of 60 in developed countries. With the aging population, the prevalence of this condition continues to increase, creating a substantial social and economic burden. In addition to reduced visual acuity, GA significantly affects patients’ quality of life.
Geographic atrophy retina OCT, together with modern digital image analysis algorithms, has become a key tool in the diagnosis, monitoring, and evaluation of OCT biomarkers predicting GA progression. OCT provides cross-sectional imaging of the retina with microscopic resolution, enabling detailed assessment of individual retinal structures—from the inner retinal layers to the RPE–Bruch’s membrane–choriocapillaris complex. This technology has enabled the transition from subjective ophthalmoscopic assessment to objective structural analysis.
The advantages of OCT in the diagnosis and monitoring of GA include its non-invasive nature, high reproducibility, ability to detect early structural changes, and accurate quantitative measurements. Structural alterations at the level of photoreceptors and the RPE often occur long before they become visible on ophthalmoscopy or fundus photography. Proper recognition of OCT biomarkers of GA is essential not only for disease diagnosis but also for personalizing treatment strategies, predicting the risk of progression, and evaluating therapeutic outcomes.
The purpose of this article is to summarize current scientific evidence on OCT biomarkers of geographic atrophy, including their morphological definition, quantitative parameters, prognostic significance, and role in monitoring disease progression. Particular attention will be given to the practical aspects of OCT in clinical practice, interpretation of longitudinal changes, and effective communication with patients regarding the expected course of the disease.
2. Main OCT Biomarkers of Geographic Atrophy
Modern understanding of GA morphology has been largely shaped by the work of international expert groups, particularly the Classification of Atrophy Meetings (CAM) Group. The CAM group proposed standardized terminology and clear OCT-based criteria for retinal atrophy, enabling harmonization of diagnostic approaches in both clinical practice and multicenter studies.
The CAM group recommends spectral-domain OCT (SD-OCT) as the preferred imaging modality for detecting GA-related changes, as it allows identification of the earliest signs of developing atrophy.
2.1 OCT Signs of Geographic Atrophy
The following three features form the basis for the standardized OCT definition of GA:
- Loss of the outer retina
- Loss of the retinal pigment epithelium (RPE) ≥250 µm in diameter
- Choroidal hypertransmission ≥250 µm in diameter
1. Loss of the Outer Retinal Layers
On OCT B-scans this manifests as:
- disruption or loss of the ellipsoid zone (EZ)
- absence of the interdigitation zone
- thinning or complete loss of the outer nuclear layer (ONL)
- thinning (atrophic changes) of the neuroepithelium above the lesion
This feature reflects the loss of photoreceptors, which are the primary functional elements responsible for central vision.
2. Loss of the Retinal Pigment Epithelium (RPE)
The CAM group established a threshold of 250 µm in the largest horizontal dimension to define clinically significant atrophy.
AI detection of RPE atrophy OCT appears as:
- absence or severe thinning of the hyperreflective RPE band
- a well-defined border between preserved and atrophic RPE
3. Choroidal Hypertransmission
Due to the loss of the RPE, light penetrates more deeply into the underlying layers, resulting in increased visualization of the choroid.
On OCT this appears as:
- Increased visibility of the choriocapillaris layer
- Clear correspondence with the area of RPE defect
Classification of Outer Retinal Atrophy Associated with AMD
- Complete RPE and outer retinal atrophy (cRORA)
- Incomplete RPE and outer retinal atrophy (iRORA)
- Complete outer retinal atrophy (cORA)
- Incomplete outer retinal atrophy (iORA)
2.2 OCT Parameters for Monitoring Geographic Atrophy
Once the diagnosis is established, OCT biomarkers predicting GA progression and quantitative monitoring of disease progression becomes critical.
1. Morphological Triad
RPE atrophy, choroidal hypertransmission, and neuroepithelial atrophy represent the hallmarks of complete retinal atrophy.
This triad defines retinal atrophy within the lesion area and allows differentiation between complete and incomplete atrophy using structural criteria.
2. Area of Geographic Atrophy (mm²)
Quantitative measurement of GA area is a key parameter in both clinical practice and research.
OCT segmentation enables highly reproducible calculation of the affected area. Modern OCT systems allow:
- automatic segmentation of atrophy boundaries
- calculation of the GA area in mm²
- comparison of measurements between visits
The annual enlargement rate of the GA area is an objective marker of disease progression and correlates with functional visual outcomes. Importantly, the GA area may increase even when visual acuity remains stable.
The area of GA served as the primary endpoint in clinical trials evaluating the intravitreal therapies Syfovre and Izervay, which were recently approved by the FDA as treatments to slow GA lesion growth.
AI-based algorithms further improve the precision and reproducibility of measurements, which is particularly important for long-term monitoring.
Modern OCT systems provide GA area measurements in mm², and comparisons between visits provide an objective measure of disease dynamics. Even when patients do not perceive changes, increasing lesion area confirms disease progression.
3. Distance Between GA Lesions and the Fovea
An important quantitative parameter is the distance between the foveal center and the nearest border of the atrophic lesion.
This parameter has direct functional significance. Decreasing distance over time correlates with declining visual function: the closer GA approaches the fovea, the higher the risk of sudden vision loss.
Patients with GA lesions approaching the fovea have a poorer prognosis and often require more intensive monitoring and therapeutic interventions.
This parameter also allows objective risk prediction and supports:
- early referral to specialized ophthalmology centers
- discussion of potential vision loss with patients
2.3 Predictors of GA Development and Progression
GA frequently develops as a consequence of drusen involution or structural alterations of the RPE.
GA lesions in AMD may arise in association with:
- certain drusen types (large or confluent drusen, reticular pseudodrusen)
- previous choroidal neovascularization
- RPE detachment or RPE tear
- refractile deposits
- vitelliform lesions
Geographic Atrophy as a Result of Drusen Involution
Drusen are localized accumulations of pathological material (photoreceptor metabolic by-products) between the RPE and Bruch’s membrane. They may change in number, size, and morphology.
Regression or disappearance of drusen, as well as structural changes observed on OCT, represent predictors of progression to GA. Regular monitoring allows early detection of potentially dangerous changes.
Types of Drusen
1. Hard Drusen
- round, well-defined yellow-white lesions
- diameter ≤63 µm
- usually asymptomatic
2. Soft Drusen
- medium: 63–125 µm
- large: >125 µm
- poorly defined borders
- may enlarge and merge
- associated with diffuse retinal dysfunction
3. Confluent Drusen
Formed by the merging of several soft drusen.
4. Drusenoid RPE Detachment
An area of confluent drusen in the macula with a diameter exceeding 350 µm according to AREDS.
5. Cuticular Drusen
- located between the RPE and Bruch’s membrane
- small in diameter but numerous
- often confluent
- steep, sloping sides (“saw-tooth” appearance)
- may disrupt RPE structure
- represent a risk factor for progression to GA
6. Reticular Pseudodrusen
- deposits located in the subretinal space between photoreceptors and the RPE
- associated with poor visual prognosis
- strongly linked with GA development
GA develops particularly rapidly in the presence of reticular pseudodrusen.
Predictors of GA Development in Eyes with Drusen
- large numbers of drusen, particularly in the central macula
- regression of drusen
- structural changes such as heterogeneous internal reflectivity
These predictors help identify patients at high risk for GA development and are valuable for optimizing monitoring intervals and potential preventive strategies.
Another predictor of faster GA lesion formation is hyperreflective foci. These are small intraretinal hyperreflective dots, often located above drusen and typically associated with local disruption of the RPE structure. They likely represent migrating RPE cells and activated microglia. A tiny blue spot is a hyperreflective foci area detected by Altris automated GA segmentation OCT:
Their presence significantly increases the risk of GA development within the next few years (in some studies up to five-fold within two years).
Clinical Importance of Predictors
Identifying high-risk patients allows clinicians to:
- individualize OCT monitoring frequency
- initiate treatment earlier
- predict functional vision loss
- discuss expected disease progression with patients in a timely manner.
Management of Geographic Atrophy and Patient Education
Management of patients with GA today extends far beyond simple observation. It involves an active, structured strategy that combines regular OCT monitoring, timely initiation of therapy, risk-factor modification, and comprehensive patient education.
The main goal is to slow disease progression and reduce the rate of atrophy expansion while preserving the central fovea for as long as possible. GA Progression quantified via Altris:
The Role of OCT
Effective GA management is impossible without high-quality OCT monitoring.
OCT enables clinicians to:
- quantify the area of atrophy
- determine the rate of lesion expansion
- measure the distance to the fovea
- analyze outer retinal layer integrity
- identify predictors of rapid progression
Monitoring is recommended every 3–6 months, and when intravitreal therapy is used, OCT should be performed before each injection to assess disease activity and lesion growth rate.
OCT also serves as a powerful motivational tool: showing patients the dynamics of structural changes helps them better understand the need for treatment and regular follow-up visits.
Patients should be informed that GA may progress without sudden visual deterioration. Structural OCT changes often precede functional vision loss, making regular examinations essential even when visual acuity appears stable.
Current Treatment Options
Intravitreal Therapy
- Izervay (avacincaptad pegol)
- Syfovre (pegcetacoplan)
For the first time in decades, FDA-approved treatments are available that slow the expansion rate of GA lesions. Although they do not restore lost vision, slowing visual decline is an important clinical goal.
Patients should clearly understand that treatment slows progression but does not restore vision. Proper expectation management improves treatment adherence and reduces disappointment.
Nutritional Supplements
Formulations based on AREDS / AREDS2 have been shown to reduce the risk of progression from intermediate AMD to advanced stages.
Patients should be informed that these supplements do not treat GA, but may have preventive value at earlier stages.
What Patients Must Understand
1. Progressive Nature of GA
GA is a chronic progressive disease. The area of atrophy almost always increases over time. The rate of progression varies depending on morphological characteristics.
Patients should understand that treatment aims to slow, not completely stop, disease progression.
2. Importance of Lifestyle
Although lifestyle modification has limited influence once GA is established, recommendations remain relevant:
- smoking cessation
- blood pressure and lipid control
- antioxidant-rich diet and omega-3 fatty acids
- regular physical activity
These factors improve overall vascular health and may reduce systemic inflammation.
3. Psychological Adaptation
Progressive central vision loss often leads to anxiety, fear of blindness, and reduced social activity.
It is important to discuss:
- low-vision aids (magnifiers, telescopic glasses, electronic magnifiers)
- support resources for people with low vision
Psychological support significantly improves adaptation and quality of life.
Patient Partnership: The Foundation of Success
Modern management of dry AMD is no longer hopeless. With approved therapies and evidence-based preventive strategies, clinicians can meaningfully influence the rate of disease progression.
However, the effectiveness of any strategy depends on collaboration between the physician and the patient.
Patient education regarding:
- the nature of the disease
- the role of regular OCT monitoring
- treatment possibilities and limitations
- the importance of lifestyle modification
is an essential component of modern GA management.
FAQs
Which OCT biomarkers are predictive of GA progression to look for?
Key biomarkers include hypertransmission defects, RPE atrophy, photoreceptor loss, ellipsoid zone disruption, hyperreflective foci, and reticular pseudodrusen. These structural changes are strongly associated with GA development and progression in AMD.
How does AI OCT help prioritize patients at risk of GA progression?
AI for GA systems identifies high-risk biomarkers and calculates progression rates, enabling clinicians to triage patients for closer monitoring or treatment.
Can AI detect multiple retinal pathologies in addition to GA?
Many platforms detect 70+ retinal pathologies and biomarkers simultaneously on OCT scans. Altris detects and quantifies 40+ retina biomarkers and 40+ pathologies.
How can AI quantify geographic atrophy on OCT scans?
AI algorithms automatically segment GA lesions and calculate lesion area, retinal layer loss, and biomarker overlap, providing objective measurements in millimeters or percentages.
Can AI OCT support treatment decisions for GA therapies?
AI can measure structural parameters such as EZ loss or RPE integrity, which may help evaluate treatment response or disease activity. Altris applies Flags to filter out the eligible patients then.
Can AI detect early GA before it becomes clinically visible?
Yes. AI models can identify subtle structural abnormalities on OCT, such as EZ disruption or early hypertransmission, enabling earlier detection of atrophy.
Which OCT metrics should be monitored to track GA progression?
Clinically relevant metrics include: GA lesion area (mm²), rate of lesion growth, distance from lesion margin to the fovea, percentage of macular involvement. AI can automatically calculate and track these parameters over time.
How to efficiently measure geographic atrophy on OCT?
To efficiently measure Geographic Atrophy on Optical Coherence Tomography (OCT), clinicians should identify key biomarkers such as RPE loss, outer retinal thinning, and choroidal hypertransmission, then quantify the atrophy area (mm²) using en-face OCT or automated segmentation tools. Tracking lesion size and its distance to the fovea over time allows accurate monitoring of disease progression. AI-assisted OCT platforms can automate detection and measurements, making longitudinal assessment faster and more consistent.
References
- Guymer RH, Rosenfeld PJ, Curcio CA, et al.
Incomplete retinal pigment epithelium and outer retinal atrophy in age-related macular degeneration: Classification of Atrophy Meeting report.
Ophthalmology.
Available at: https://pubmed.ncbi.nlm.nih.gov/38387826/ - Natural history and progression of geographic atrophy in AMD.
ScienceDirect.
Available at: https://www.sciencedirect.com/science/article/pii/S2468653023006681 - OCT Spotlight: Characterizing Geographic Atrophy Development and Progression.
Retina Today.
Available at: https://retinatoday.com/articles/2025-apr/oct-spotlight-characterizing-ga-development-and-progression - Automated monitoring of geographic atrophy using OCT imaging.
Scientific Reports.
Available at: https://www.nature.com/articles/s41598-023-34139-2 - Classification of Atrophy Meeting (CAM) consensus for OCT-based atrophy classification in AMD.
American Academy of Ophthalmology Journal.
Available at: https://www.aaojournal.org/article/S0161-6420(17)31703-7/abstract - Identifying Geographic Atrophy Biomarkers.
Optometric Management.
Available at: https://www.optometricmanagement.com/issues/2025/october/identifying-geographic-atrophy-biomarkers/ - FDA Approval Announcement for Izervay (avacincaptad pegol).
Astellas Pharma Newsroom.
Available at:
https://newsroom.astellas.com/2023-08-05-Iveric-Bio-Receives-U-S-FDA-Approval-for-IZERVAY-TM-avacincaptad-pegol-intravitreal-solution-,-a-New-Treatment-for-Geographic-Atrophy
-
Altris AI Receives Health Canada Approval

 Altris Inc.
Altris Inc.
Altris AI Receives Health Canada Approval, Reinforcing Its Position as a Globally Trusted AI Decision Support Platform for OCT Analysis
Regulatory clearance marks a pivotal milestone in Altris AI’s international expansion and its mission to bring clinical-grade AI to eye care worldwide.
10 March 2026 — Altris AI, a leading provider of AI-powered decision support for optical coherence tomography (OCT) analysis, today announced it has received approval from Health Canada | Santé Canada, Canada’s federal health regulatory authority. This clearance represents a significant step forward in the company’s global growth strategy and its commitment to meeting the highest standards of medical device safety and clinical reliability.
For a company scaling across international markets, regulatory approvals are far more than administrative milestones — they are foundational growth enablers. Health Canada approval strengthens Altris AI’s international positioning, opens new pathways for future regulatory submissions across key markets, and delivers a clear signal to the global healthcare community: Altris AI is built for real-world clinical practice.
The approval confirms that Altris AI’s clinical and technical validation withstands the rigorous scrutiny of Health Canada’s regulatory review process, which evaluated the platform across five critical dimensions: clinical evidence supporting efficacy and safety claims; risk management protocols; cybersecurity safeguards; quality management systems; and intended use claims. Each of these pillars reflects the standard that modern AI-driven medical devices must meet before being trusted in clinical settings.
Altris AI’s platform serves optometrists, ophthalmologists, and pharmaceutical organizations by providing intelligent, reliable support for interpreting OCT scans — one of the most widely used diagnostic tools in eye care. By surfacing clinically relevant findings with speed and precision, Altris AI empowers clinicians to make more informed decisions, improve patient outcomes, and increase the efficiency of ophthalmic workflows.

“This approval is external confirmation that our platform meets the standards required for medical-grade AI,” said Maria Znamenska, Chief Medical Officer at Altris AI. “Health Canada’s review is thorough, evidence-based, and internationally respected. Receiving this clearance validates not just our technology, but the entire approach we’ve taken — building AI that clinicians can trust, in environments where accuracy is not optional.”
The Health Canada clearance follows a broader regulatory strategy that positions Altris AI as a compliant, audit-ready platform for healthcare systems worldwide. As global regulators increasingly scrutinize AI in medical devices, early and consistent compliance across multiple jurisdictions will become a decisive competitive differentiator.
Altris AI’s mission is to accelerate the transition of AI in eye care from innovation to infrastructure — not as a replacement for clinical expertise, but as a trusted decision-support layer that elevates the standard of care across every point of practice.
About Altris AI Altris AI is an AI Decision Support platform for OCT analysis, designed to support optometry, ophthalmology, and pharma with clinically validated, regulatory-compliant technology. The company is committed to expanding access to intelligent eye care diagnostics globally.
-
AI in Optometry: 5 Real Applications
Maria Znamenska
9 min.Highlights: AI in optometry is revolutionizing clinical decision-making by allowing eye care professionals to analyse B-scans with greater precision, consistency, and confidence right at the point of care.
- AI for fundus analysis is another way to automatically evaluate fundus scans in an optimized way throughout all devices.
- AI-driven deep learning algorithms can detect and quantify retinal and optic nerve pathologies in OCT images, enabling earlier identification of diseases such as glaucoma, age-related macular degeneration (AMD), and other retinal conditions.
- AI-assisted analysis enhances clinical efficiency by helping clinicians triage scans, monitor disease progression over time, and focus on clinically significant findings, rather than relying solely on manual scan reviews.
- Other AI-powered tools provide objective visual insights for clinicians and patients, improving the accuracy of triage and treatment monitoring and enhancing patients’ understanding of retinal health.
- AI enables optometrists to manage more complex ocular cases in primary care, facilitating earlier detection, risk stratification, and informed referral decisions based on objective insights.
- AI chatbots in optometry inform about eye symptoms, guide whether to seek care (urgent vs. routine), suggest possible conditions, support patients and help decide next steps, etc. Or manage eye care specialists’ daily routine.
Introduction
Artificial intelligence is increasingly shaping healthcare by enhancing clinicians’ ability to interpret complex medical data and make earlier, more informed decisions. AI in optometry is especially important in OCT imaging, where it is essential to correctly interpret subtle structural changes to identify eye disorders early.
AI for optometrists can therefore more reliably and consistently detect and track retinal and optic nerve disorders by integrating deep learning into OCT data. In routine optometric practice, risk management and referral decision-making are enhanced by converting OCT images into understandable, actionable findings.
Discover how optometry AI tools redefine optometry by improving diagnostic accuracy, clinical efficiency, and the quality of patient care in 5 real cases.
1. AI Decision Support for OCT Analysis
One of the most effective AI applications in optometry is AI decision support for OCT analysis.
AI decision-support systems are increasingly applied to OCT imaging to assist optometrists in interpreting complex retinal and optic nerve data. Here’s one of the real cases when AI brings ultimate use to practitioners:
Thus, AI-powered platforms like Altris use deep learning algorithms to automatically detect and quantify structural changes, highlight areas of concern, and track progression over time via an AI OCT pathology detection tool.
By analysing patterns across large datasets of retinal scans, the system can flag subtle abnormalities that may be difficult to identify manually, segment them automatically, and provide structured, visual insights that help clinicians make more informed, consistent decisions while monitoring patient eye health. It does everything eye care specialists do, but faster, error-free, and unbiased.
In particular, Altris AI also applies deep learning to OCT scans to automatically detect and highlight complex retinal and optic nerve changes.
The system quantifies abnormalities, tracks progression over time, and provides visual insights that help optometrists interpret scans more accurately and consistently, again supporting far more informed clinical decisions.
2. AI for Fundus Analysis
AI for Fundus Analysis is another way to automatically evaluate fundus scans in an optimized way throughout all OCT devices. Among the top 3 AI software solutions for fundus imaging, there are:
Auroraa AI (Optomed) is an advanced artificial intelligence platform integrated with Optomed’s handheld and tabletop fundus cameras, designed to detect multiple retinal abnormalities including diabetic retinopathy, glaucoma, and age‑related macular degeneration; it provides immediate, automated screening results to support clinicians and improve early disease detection.
Beammed’s AI‑powered fundus cameras pair intelligent image analysis with portable retinal imaging to enable early detection of diabetic retinopathy and other retinal conditions, leveraging deep learning algorithms to highlight pathology and help streamline screening programs.
Cybersight AI (Orbis) offers an AI‑driven diagnostic support tool focused on interpreting fundus images to assist eye care providers in low‑resource settings and telemedicine programs, combining machine learning with expert clinical guidance to improve access to retinal disease screening globally. Here’s how fundus tool may look like:
Such systems provide severity scores, highlight areas of concern, and track changes over time, giving clinicians objective, reproducible insights to support their decisions. Since AI can detect early signs of conditions like glaucoma, diabetic retinopathy, and age-related macular degeneration, it often spots subtle changes that are hard to see with the naked eye.
3. AI for Automated Visit Scheduling
AI‑powered appointment scheduling systems are digital tools that, alongside any modern AI OCT pathology detection tool or similar, use artificial intelligence — including natural language processing (NLP), predictive analytics, machine learning, and automated communication — to handle clinical scheduling tasks usually done manually by staff. These tools can:
- let patients self‑schedule online, by chat, voice, or text at any time,
- automatically confirm, remind, reschedule, or cancel appointments,
- optimize schedules based on provider availability and patient needs, and
- predict and prevent clinic inefficiencies such as no‑shows.
In essence, the system acts as a digital receptionist and smart scheduler, integrating with clinic practice management software, EHRs, and CRM systems to manage workflows seamlessly. Best EHR systems include:

Elation EHR is a cloud-based electronic health record designed primarily for independent primary care practices. It focuses on simplifying clinical workflows, documentation, and patient engagement, with strong charting tools and longitudinal patient records. It’s used to help physicians deliver personalized care while reducing administrative burden.
Epic is one of the most widely used enterprise EHR systems globally, typically implemented by large hospitals and health systems. It integrates clinical, administrative, and billing functions into a single platform, supporting everything from patient records to population health management. It’s used to coordinate care at scale and improve interoperability across departments and organizations.
Tebra combines electronic health records with practice management, billing, and patient communication tools, targeting small to mid-sized medical practices. It streamlines front-office and clinical operations in one system, helping practices manage scheduling, documentation, and revenue cycle efficiently.
Nextech EHR is a specialty-focused EHR designed for fields like ophthalmology, dermatology, and plastic surgery. It includes tailored templates, imaging integration, and workflow tools specific to these specialties. It’s used to enhance clinical efficiency and documentation accuracy in specialized practices.
InSync EHR is a cloud-based EHR built for behavioral health and therapy practices. It supports telehealth, scheduling, documentation, and billing, with features tailored to mental health workflows. It’s used to improve care coordination and streamline operations for therapists and behavioral health providers.
These tools are designed to improve operational efficiency, reduce administrative burden, and enhance the patient journey in healthcare settings. They offer 24/7 availability, personalized booking flows, and real-time updates, making them a powerful part of your workflow.
ModMed EMA (Electronic Medical Assistant) is an AI-driven, specialty-specific EHR developed by Modernizing Medicine. It uses structured data and adaptive templates to support clinical decision-making and documentation. It’s used by specialists to increase efficiency, improve outcomes, and reduce time spent on manual data entry.
“Up to 71% of U.S. hospitals now use predictive AI technologies for scheduling and related automation.”
Indeed, AI in optometry for appointments, self-scheduling, and other administrative tasks can optimize routine workflows and offer a range of benefits for both opticians and their visitors. They:
- Remove Administrative Burden
AI takes over repetitive scheduling tasks — booking, confirmations, cancellations, preregistration, and follow‑ups — freeing front‑desk staff and nurses to focus on patient care rather than paperwork.
Historically, nurse managers and front‑desk staff can spend up to 40% of their day on scheduling tasks, and automating this saves hours of labour.
- Provide 24/7 Booking & Patient Flexibility
Patients no longer have to call during office hours. AI scheduling tools enable self‑service booking, changes, and cancellations at any time via chatbots, voice interfaces, or online portals.
This has become especially crucial, as 40% of healthcare appointments are requested outside normal business hours — times when traditional phone booking is impossible.
- Reduce No‑Shows & Better Attendance
Automated reminders — via SMS, email, or voice — consistently reduce no‑show rates, which can otherwise waste clinic time and revenue. Clinics using these tools have reported:
-
No‑shows dropped from 20% to as low as 7% with automated reminders.
-
In some settings, AI virtual assistants reduced missed visits by up to ~73%.
AI can also predict patients likely to skip visits and prompt engagement before issues arise.
- Enhance Resource Use
Instead of manually guessing who should be booked and where, such AI in optometry:
✔ matches patients with the right clinician,
✔ avoids double bookings and schedule conflicts,
✔ spreads appointments evenly to reduce bottlenecks, and
✔ improves utilization of staff time and rooms.
AI scheduling can increase provider utilization by 15–25% and reduce wait times by 15–30%.
- Improve Patient Experience
Patients appreciate convenience. Access to online or chatbot booking correlates with improved satisfaction — one study showed satisfaction scores can rise by over 20% when patients can self‑manage appointments.
AI also reduces inbound phone volume by 25–40%, allowing clinics to serve patients more efficiently.
For instance, Tele-optometry decision support that offers
- AI pre-analyses remote exams
- Flags cases requiring in-person referral
- Supports non-specialist reviewers
has the following workflow impact:
- Scales remote care
- Consistent quality
- Faster review cycles
Used in:
- Large optometry chains
- Retail vision centres
- Franchise-based practices
- Rural clinics
- Community health centres
- Mobile eye clinics, etc.
4. AI Workflow & Practice Optimization
So, AI-assisted OCT analysis has become helpful in retina & glaucoma screening, in follow-ups, progression tracking, and other workflows. Meaning, what happens with OCT with the help of an AI OCT pathology detection tool is helpful in many ways:
- OCT scans are automatically analysed
- Pathologies are flagged (fluid, thinning, progression risk, etc.)
- Clinicians review AI output before raw scans.
So, they get
- Faster exam review
- Fewer missed subtle findings
- Consistent interpretation across doctors, etc.
But real-world AI applications in optometry for clinic management do not stop there: scheduling, reminders, patient triage, administrative automation, analytics, and beyond may also be supported by specific optometry AI tools. Here are a few examples.
AI triage tools for urgent eye issues
- AI pre-screens OCT/fundus images
- Exams are auto-prioritized by severity
- High-risk patients are flagged before the visit
Workflow impact:
- Smarter scheduling
- Faster routing to specialists
- Less cognitive load on staff
Used in:
- High-volume optometry chains
- Tele-optometry services
An example of AI diagnostic software for optometry and ophthalmology can be IDx-DR AI Diagnostic System for Detecting Diabetic Retinopathy.
Automated appointment reminders
Automated appointment reminders are AI- or rules-based systems, not yet independent chatbots or AI assistants, that automatically notify patients about upcoming eye exams via SMS, email, WhatsApp, or voice calls, without staff involvement.
They usually trigger:
- 7 days before (prep + reschedule window)
- 48–72 hours before (confirmation)
- 24 hours or same day (final reminder)
which makes them still a new generation of automation tools for eye care. Well-designed systems, like the majority of AI in optometry tools, support:
- HIPAA / GDPR-compliant messaging
- No clinical advice in reminders
- Audit logs of sent communications
- Opt-out controls
This makes them safe for both routine and medical eye care appointments.
For example: EyeCloudPro
But why do no-shows happen in optometry? Like in any other service sphere, there are real reasons why:
- Routine exams feel “non-urgent.”
- Long booking lead times (2–6 weeks)
- Patients forget dilation/prep requirements
- Elderly patients miss calls or misremember dates
- Parents forget pediatric appointments
- No easy way to confirm or reschedule
Across outpatient care (including optometry), automated reminders typically achieve:
- 20–40% reduction in no-shows
- 5–10% increase in appointment confirmations
- Up to 30% fewer last-minute cancellations
- 1–2 hours/day staff time saved (no manual calls)
In optometry specifically, clinics with long routine exam cycles often see results closer to the upper end of those ranges. What automated reminders do here is directly target forgetfulness + reduce friction. No ordinary staff can do that to such an extent. But AI can.
Therefore, by keeping patients aware, ready, and involved, automated appointment reminders help optometry clinics reduce no-show rates. Practices may increase patient flow, maximize chair time, and enhance attendance by providing timely, customized notifications through preferred channels—all without adding to the administrative burden.
Patient communication and optometrists’ education appsPatient communication, as well as optometrist education systems and applications, for mobile and desktop usage, support clearer understanding, better engagement, and more consistent care delivery.
For example: Chatbots in Healthcare from Capacity
These tools help patients understand their eye health and treatment plans, while enabling optometrists to stay informed through structured education, clinical updates, and decision-support resources—improving outcomes without increasing chair time:
- AI translates OCT findings into plain language
- Visual overlays show “what changed” and “why it matters.”
- Used chairside or via patient portal
Workflow impact:
- Better patient understanding
- Higher treatment acceptance
- Shorter explanation time per visit
Used in
- Routine eye exams
- OCT review appointments
- Retina & glaucoma visits
- Anti-VEGF treatment discussions
- Glaucoma therapy initiation
- Long-term monitoring plans, etc.
Altris Education application, as an example of a unique tool specifically designed for eye care specialists’ training:
5. Chatbots for Consultation
A separate category is AI chatbots and virtual assistants that help with patient follow-up, education, and communication, improving day-to-day patient communication and more. With the AI Help Assistant feature, you can create an AI chatbot trained on your specific content from any platform you like. Chatbots for consultation in optometry offer clear, practical benefits for both clinics and patients:
- 24/7 Q&A
- Absolutely personalized follow-up instructions
- Higher patients satisfaction rate
Furthermore, they provide instant, 24/7 responses to the most common eye-care questions, helping patients understand symptoms, prepare for visits, and follow post-exam instructions without even waiting for staff availability.
Chatbots can assist with pre-consultation triage by gathering symptoms, visual complaints, and medical history, allowing optometrists to focus on higher-value clinical tasks.
They also improve patient engagement and adherence by delivering personalized education, reminders, and care instructions in simple, easy-to-understand language.
Overall, optometry chatbots dramatically reduce administrative workload, shorten response times, and support more efficient, patient-centered care while maintaining consistent communication quality.
Types of Chatbots in Eye Care & Optometry
1. Symptom & Triage Chatbots
These ask users about eye symptoms, guide whether to seek care (urgent vs. routine), suggest possible conditions, and help decide next steps. Example: Ada Health
A study published in Eye showed that large‑language‑model‑based chatbots (e.g., ChatGPT) could answer common ophthalmology questions with high accuracy and clarity — scoring higher than alternative generative models for diagnostic and triage‑related queries (accuracy and comprehensiveness metrics showed ChatGPT did well on standard patient questions).
Another clinical evaluation found that AI (GPT‑4) correctly identified the appropriate diagnosis among the top three options in up to 93% of ophthalmology cases and correctly assessed urgency levels in most cases — performance comparable to that of trainees.
2. Real‑World Chatbots for Eye Care
The patient describes eye symptoms and uploads images (e.g., photos or OCT scans).
An AI assistant organizes symptoms and images for review, then a real ophthalmologist chats with the patient to guide care. Key inputs here:
- Collect symptoms in natural language
- Translate or clarify reports
- Help the clinician interpret visuals and decide next steps
It combines AI symptom intake with real human consultation, making remote triage efficient.
AI in optometry real chatbot examples:
- WebEyeClinic / Visio — symptom intake & remote clinician chat
- VisionCare Assistant — eye health guidance
- DocsBot AI — practice support
- Custom AI agents via Voiceflow — administrative automation, etc.
3. DocsBot AI for Optometry Services
Practice‑focused chatbot helping clinics answer FAQs, provide pre‑appointment instructions, and automate patient engagement. Benefits:
• Instant responses to common patient queries
• 24/7 availability for basic information
• Can free up staff time by handling routine communication, such as allowing self-booking, etc.“Patients express high satisfaction with AI self‑booking capabilities (up to 85% positive ratings).”
Here are some more real AI chatbot applications in eye care:
Tool / Platform Primary Focus DocsBot AI Patient FAQs & practice engagement ThriveDesk AI AI customer support for optometry Voiceflow AI Agent Custom appointment/scheduling chatbot MedReception AI Manage eye exams, contact lens orders, and optical retail coordination OptoAI AI Assistant Knowledge and clinical support agent Pod AI AI phone/communication agent As highlighted, there is a wide array of chatbot types in optometry, ranging from patient-facing virtual assistants to AI-powered communication platforms.
With features such as automated appointment scheduling, pre-visit coaching, FAQ handling, 24/7 patient engagement, and basic clinical decision support, these optometry AI systems offer substantial value.
By streamlining administrative tasks and improving patient education, these AI chatbots free up clinicians’ time to focus on direct care.
Overall, the integration of AI-driven chatbots is revolutionizing the delivery of eye care. They enhance operational efficiency, reduce missed appointments, support timely patient triage, and improve adherence to care plans. By combining automation with intelligent decision support, AI not only optimizes clinic workflows but also elevates patient outcomes and satisfaction, marking a transformative shift in modern optometry practice.
Conclusion
AI is rapidly becoming a practical and valuable tool in optometry, particularly for analysing OCT imaging. By enabling more consistent interpretation of complex retinal and optic nerve data, AI in optometry supports earlier identification of disease-related changes, more efficient triage, and improved longitudinal monitoring.
Beyond clinical efficiency, AI enhances patient communication by translating OCT findings into clear visual insights, supporting better understanding and engagement. As a result, optometrists are better equipped to manage more complex cases in primary care, make informed referral decisions, and deliver higher-quality, data-informed eye care—positioning AI as a meaningful complement to clinical expertise rather than a replacement.
FAQs
Is AI for optometry safe?
AI in optometry is generally safe when it is properly validated, regulated, and used as a clinical support tool rather than a replacement for professional judgment. It can improve screening accuracy, enable earlier detection of eye diseases, and streamline workflows, but it also carries risks such as diagnostic errors, data privacy concerns, and bias if systems are poorly trained or over-relied upon. For safe use, optometrists must remain responsible for final decisions; patients should be informed when AI is involved; and tools should comply with medical regulations (such as FDA or CE approval) and data protection standards, such as GDPR or similar, depending on the region.
What’s an AI OCT pathology detection tool?
An AI OCT pathology detection tool is a software system that uses artificial intelligence to analyse optical coherence tomography (OCT) images of the eye and automatically identify signs of disease, such as macular degeneration, glaucoma, or diabetic retinopathy; it assists clinicians by highlighting abnormalities and suggesting potential diagnoses, but it is designed to support—rather than replace—professional interpretation, and its safety and effectiveness depend on proper validation, regulatory approval, and clinician oversight.
Can AI help reduce no-shows and long wait times in an optometry practice?
Yes. AI applications in optometry are limitless. AI can help reduce no-shows and long wait times in optometry practices by supporting appointment scheduling, reminders, and workflow optimization—such as identifying scheduling patterns, highlighting bottlenecks, and enabling more efficient patient flow—while assisting staff with better resource planning and communication.
What can chatbots and AI assistants do for an optometry practice?
Chatbots and AI assistants can help an optometry practice automate patient communication, streamline scheduling, and improve clinical efficiency by answering FAQs 24/7, booking and confirming appointments, sending reminders, pre-screening patients with symptom checkers, collecting medical history before visits, and triaging urgent cases. They can also support front-desk staff by handling insurance questions, guiding patients to the right services (e.g., OCT, glaucoma screening, contact lens exams), following up after visits, and reactivating inactive patients through personalized messaging. Internally, AI in optometry assistants can summarize patient data, flag high-risk cases, analyse trends in no-shows or referrals, and help with marketing automation — ultimately reducing administrative workload, improving patient satisfaction, and increasing practice revenue.
What kinds of clinical or diagnostic support can AI provide in eye exams?
AI can support eye exams by assisting with image review, pattern recognition, and data organization—such as highlighting features in retinal images, supporting consistency in exam review, and providing quantitative reference information—while remaining a complement to clinician judgment rather than a replacement for clinical decision-making.
How can AI increase optical revenue and overall patient satisfaction?
AI in optometry can increase optical revenue and patient satisfaction by helping practices streamline workflows, reduce wait times, support personalized patient communication, and enhance the in-practice experience through clearer visualization and education tools—leading to more efficient operations, improved engagement, and higher-quality service delivery.
References:
Luhmann, U. F. O. (2015). Innate immunity in age-related retinal degeneration. Acta Ophthalmologica. https://doi.org/10.1111/j.1755-3768.2015.0144
https://remidio.us/solutions/teleophthalmology-telehealth/
https://medpick.in/product/idx-dr-ai-diagnostic-system-for-detecting-diabetic-retinopathy/
https://www.rcophth.ac.uk/academic-and-research/eye-journal/
https://webeyeclinic.com/how-it-works/
https://docsbot.ai/industry/optometry-services
https://www.voiceflow.com/ai/optometrists
https://healthus.ai/service/ai-chatbot-appointment-module/
https://arxiv.org/abs/2511.09394
https://ajbsr.net/data/uploads/6387.pdf
-
Altris becomes the winner of VSP Vision Challenge at Vision Expo
 Altris Inc.
1 min.
Altris Inc.
1 min.ORLANDO, FL — Altris, an IMS for OCT analysis with ROU AI models, has been named the Judge’s Winner of the 2026 VSP Vision Innovation Challenge, one of the eyecare industry’s most prestigious startup competitions. The award was presented live on March 13, 2026, on the Innovation Stage at Vision Expo inside the Orange County Convention Center in Orlando, Florida.
Produced by RX and The Vision Council in collaboration with VSP Vision™, the 2026 VSP Vision Innovation Challenge drew applications from companies around the globe — more than half of which were venture-backed, collectively representing over $300 million in funding. After a rigorous selection process, Altris AI was chosen as one of four finalists and participated in an intensive four-week startup bootcamp before delivering a live pitch to a distinguished panel of industry judges.
Judges recognized Altris for its clinical impact, technological sophistication, and potential to fundamentally transform the eyecare experience. The judging panel represented a diverse cross-section of industry leaders, including executives, clinicians, and investors.
“Winning the VSP Vision Innovation Challenge is a powerful validation of what we’re building at Altris AI. Our mission is to put the most advanced retinal intelligence in the hands of every eye care professional — and this recognition from a world-class panel of judges confirms that the industry is ready for this transformation.”
Altris AI CEO, Andrey Kuropyatnyk
About Altris
Altris AI serves as a “second set of eyes” for eye care specialists, identifying more than 70 retinal biomarkers from optical coherence tomography (OCT) scans ( AI models are used for Research Use Only). The platform enables providers to match patients to the most appropriate treatments, devices, and clinical trials with objective, data-driven precision. Altris system is FDA-cleared and HIPAA-compliant, and integrates seamlessly with OCT scanners from nine major manufacturers.
By combining advanced deep learning algorithms with a clinically intuitive interface, Altris AI reduces diagnostic variability, supports earlier detection of sight-threatening conditions, and frees eye care professionals to focus on what matters most: patient outcomes.
About the VSP Vision Innovation Challenge
The VSP Vision Innovation Challenge is a global competition designed to source, support, and accelerate early-stage startups and technologies advancing the eyecare experience. This year’s finalists represented a broad spectrum of innovation — from AI-driven diagnostics and exam automation to digital education and accessibility-focused smart solutions.
In addition to pitching live, finalists exhibited at Vision Expo’s Innovation Center, a dedicated emerging-technology destination featuring more than 20 next-generation startups spanning AI, augmented and virtual reality, and advanced diagnostics.
“Innovation in eyecare is accelerating, which is why it’s crucial for the industry to stay actively engaged. We launched the VSP Vision Innovation Challenge to connect emerging technologies with the stakeholders they aim to serve, and this year is no exception. We’re proud to support solutions that advance care for both providers and patients.”
— Will Flanagan, Head of VSP Global Innovation Center Programs and Partnerships
Looking Ahead
With this recognition, Altris AI continues to accelerate its mission of making retinal AI accessible to every eye care professional. The company will leverage the visibility and industry connections gained from the challenge to deepen partnerships with providers, expand clinical integrations, and advance its platform’s capabilities.
The next VSP Vision Innovation Challenge will take place at Vision Expo 2027, scheduled for March 10–13 in Las Vegas. Applications are expected to open later this fall.
About Altris Inc.
Altris AI is a clinical-grade SaaS platform that empowers eye care specialists with AI-driven retinal analysis. By identifying 70+ retinal biomarkers from OCT scans, Altris AI helps providers deliver more precise, evidence-based care. The platform is FDA-approved, HIPAA-compliant, and compatible with OCT devices from nine leading manufacturers.
-
Drusen on OCT: Detection, quantification, and tracking
 Maria Znamenska
5 min.
Maria Znamenska
5 min.Introduction
Drusen remains one of the main biomarkers of age-related macular degeneration (AMD). They play a prognostic role and reflect the stage of the disease. Distinguishing drusen parameters provides a personalized risk profile for the transition to geographic atrophy or neovascular AMD. Everyone working with AMD patients should know how to detect, quantify, and track drusen on OCT.
What are the types of drusen?
Drusen are accumulations of pathological material of lipid-protein nature, localized under the PES. They reflect impaired transport and exchange between the retinal pigment epithelium and Bruch’s membrane. Historically, they are divided into hard, soft, reticular pseudodruses (or subretinal drusenoid deposits) and other less common types (confluent, pachidruses) as well as other retinal OCT biomarkers for drusen segmentation.
Hard drusen
On ophthalmoscopy, they are small, rounded, clearly delineated foci of yellowish-white color. On OCT, they look like local deposits of hyperreflective material under the PES with a diameter of no more than 63 microns. In small quantities (up to 8), they are not a sign of pathology. They are asymptomatic in most patients.
Soft drusen
Soft drusen are larger than hard drusen and appear as extensive foci with blurred edges on the fundus. On OCT, they are dome-shaped and elevated above the PES and are divided into medium (63-125 μm) and large (more than 125 μm) in size. They are more strongly associated with AMD progression, especially when accompanied by pigmentary abnormalities and other OCT biomarkers (hyperreflective foci, destruction of the ellipsoidal zone, etc.). Soft drusen can enlarge and merge. An area of merging drusen with a diameter exceeding 350 μm is called a drusenoid detachment of the PES.
Soft drusen detected by Altris IMS. AI models are for Research Use Only. Not for use in diagnostic purposes.
Confluent drusen
These are multiple small deposits under the PES, which can occur in relatively young patients; on FAG they often show a “starry sky” appearance. On OCT, there are multiple small symmetrical elevations of the PES, small in diameter (like hard drusen), but more numerous, prone to merging. The course is variable: some patients maintain a stable course for years, some have an increased risk of complications and transition to the late stages of AMD.
Reticular pseudodrusen (or subretinal drusenoid deposits)
They differ fundamentally in their localization, being located above the PES (in the subretinal space). They contain some common proteins with soft drusen, but differ in lipid composition. Due to their close location to the important photoreceptor layer, they are more often combined with a decrease in visual function, and also carry a higher risk of progression to late AMD (especially characterized by a rapid transition to geographic atrophy (GA) and the development of macular neovascularization (MNV) type 3).
What are the levels of drusen?
The AREDS size classification is still useful in clinical practice: small <63 μm, medium 63–124 μm, large ≥125 μm. Analyses confirm that the 5-year risk of progression to late AMD increases with the number and size of drusen in both eyes and especially with the presence of reticular pseudodrusen. In the NICE guidance for the management of patients with AMD (2018), the risk of progression also depends on the size and type of drusen, as well as the presence of associated pathological changes (pigmentary abnormalities, vitelliform deposits).
The OCT era has added powerful quantitative metrics with AI for drusen measurement and monitoring:
- drusen height (μm),
- area (mm²),
- volume (mm³),
- topography (central ring within 1.5 mm; parafovea 3–5 mm),
- dynamics of changes and associated biomarkers (hyperreflective foci, ellipsoidal zone disruption, presence of hypertransmission zones, etc.).
A practically significant increase in the volume of drusen in the macular region over a year/two correlates with structural and functional deterioration (destructive changes in the photoreceptor layer, changes in ONL thickness, visual acuity). Data from multicenter projects (such as MACUSTAR) confirm the repeatability of measurements and the possibility of comparison between devices, provided that the correct algorithms are used.
What do drusen look like on OCT?
On B-scan OCT, classic hard and soft drusen are localized deposits of hyperreflective material between the PES and Bruch’s membrane (under the PES). Reflectivity can be uniform or heterogeneous depending on the structure and stage of development. Reticular pseudodruses are localized between the photoreceptor layer and the PES (above the PES) – this is the key difference from conventional drusen. On OCT images, they appear as tubercles in the subretinal space that remodel the outer layers of the retina (in particular, the ellipsoidal zone), and on en face, they are visualized as punctate structures, usually connected in a mesh pattern.

A: Soft drusen. B: Hard drusen (Source) Another classic white and black scan
In addition to the drusen themselves, clinically significant are hyperreflective foci, destruction of the ellipsoidal zone, thinning of the outer layers/ONL, formation of hyperreflective foci in OCT or geographic atrophy with the effect of hypertransmission – it is the combinations of these features that form prognostic models of the transition of intermediate AMD to late stages. The combination of these biomarkers consistently exceeds single morphometric thresholds.

En Face Optical Coherence Tomography Illustration of the Trizonal Distribution of Drusen and Subretinal Drusenoid Deposits in the Macula (Source)
As we can see, en face and linear OCT scans help to differentiate different types of drusen and track their progression dynamics. Modern deep learning models for AI drusen examination and en face analysis, like Altris.AI, reliably detect and segment classic drusen from subretinal drusenoid deposits, improving repeatability and reporting speed. You may see the difference from the classic white and black image analysis here:

Confluent drusen are highlighted by Altris IMS. AI models are used for Research Use Only. Not for use in Diagnostic Purposes.
How to measure drusen size?
Here we can find how drusen are measured:
1) Classical size scale (AREDS):
Orientation on diameter or equivalent on planar reconstructions: <63, 63–124, ≥125 μm. Convenient, but does not take volume/height or topography into account.
2) Quantitative OCT analysis of PES elevation:
On ZEISS CIRRUS instruments, the Advanced RPE Analysis module automatically calculates the area and volume of PES elevation in standard 3 and 5 mm rings around the fovea; the minimum height that the system consistently includes in quantitative results is about 19–20 μm. This provides repeatable metrics and a common “language of numbers” for clinical and research purposes.
3) Morphometric rule for differentiation of drusen and drusenoid detachment of PES:
By basal width: <350 μm – drusen, ≥350 μm drusenoid detachment of PES.
4) AI segmentation and 3D morphometry:
Deep networks segment Bruch’s membrane, PES, and ellipsoidal zone, as well as PES elevation on OCT, calculating drusen height/area/volume and generating dynamics maps. Validation work in 2023–2025 will demonstrate robustness between different OCT devices, which is critical for multicenter networks. Besides, you may track drusen progression on OCT AI tool and stay informed ahead of time to prevent more severe pathology changes in advance.
Can drusen exist without macular degeneration?
Yes, and this is possible in the following cases.
Small (<63 μm) single drusen may occur in the elderly in the absence of other signs of AMD and concomitant risk biomarkers (hyperreflective foci, ellipsoidal zone abnormalities). In this phenotype, the 5-year risk of progression is low; routine monitoring at an interval of 1 time per year is sufficient, if possible, with recording quantitative indicators on OCT (volume/area of PES elevation) for comparison in dynamics. The patient should be informed that the fact of “small drusen” alone does not equal a diagnosis of AMD and does not require treatment, but it is advisable to maintain lifestyle modification (blood pressure control, smoking cessation, a healthy diet).
Confluent drusen are sometimes found in younger patients; they do not always fit into the classic models of AMD. Tactics – individual observation with an emphasis on high-quality OCT documentation (the same scan and control of concomitant biomarkers). In the absence of “red flags”, a 6-12 month follow-up interval is sufficient.

Understanding Macular Degeneration (Source)
Hereditary dystrophies (EFEMP1-related; associated phenotypes are Doyne’s cellular degeneration of the retina and Leventis’ malady) form drusen-like deposits without the typical pathogenesis inherent in AMD. They have an autosomal dominant inheritance pattern and are characterized by yellow-white deposits, like drusen, accumulating under the PES, often in the peripapillary zone. The clinical picture may include gradual vision loss, impaired contrast sensitivity, or metamorphopsia. In this case, timely detection of the phenotype (age of onset, family history, symmetry, characteristic fundus appearance) and referral for medical and genetic counseling with a subsequent individual follow-up plan, including monitoring of possible complications (neovascularization, atrophic changes).
Drusen vs. drusenoid detachment of PES
Drusen are local elevations of PES above Bruch’s membrane due to deposits of pathological material under PES. Usually multiple, of different diameters, with a tendency to merge with the formation of larger, topographically continuous areas of PES elevation.
Drusenoid detachment of the pigment epithelium is formed from a larger conglomerate of drusenoid material, which in turn is formed as a result of the fusion of drusen.

Another differentiating drusen and drusenoid deposits subtypes on multimodal imaging samples
On B-scan OCT, it has smooth edges, uneven reflectivity, and often retains communication with neighboring drusen. On en face visualization, a conglomerate of elevation is visible, which corresponds to the zone of changes in the PES-Bruch’s membrane complex. In the absence of fluid inside the lesion, we are talking about drusenoid detachment of PES; if homogeneous hyporeflectivity is visualized under PES, this is serous detachment of PES, and if there are signs of a neovascular membrane according to OCTA or FAG, this is fibrovascular detachment of PES. Therefore, in doubtful cases, it is advisable to add OCTA to exclude hidden MNV.
The main morphometric rule: basal width ≥350 μm (in the horizontal projection of the OCT slice favors drusenoid detachment of PES. In some situations, we also pay attention to the content (serous/optically empty space, signs of vascularization), PES profile, and associated biomarkers, since PES detachment is more often associated with the risk of transition to HA or the formation of neovascularization.
What is the best treatment for drusen?
Drusen are not treated as a separate nosology. They are a structural biomarker of AMD, and also have prognostic value for assessing the further development and rate of progression of the disease.
Optimal tactics for detecting drusen:
Optimal tactics for detecting drusen may include the following
Risk modification:
- smoking cessation,
- blood pressure control,
- metabolic profile,
- diet.
Dietary supplements based on AREDS 2:
- taking antioxidant complexes (lutein, zeaxanthin, vitamins C and E, zinc, copper) reduces the risk of transition to late AMD by approximately 25% within 5 years (according to AREDS 2).
Quantitative monitoring on OCT:
- record the volume/area/height of drusen and their dynamics, distinguish between drusen types, detect other concomitant signs of AMD progression (hyperreflective foci, destructive changes in the ellipsoidal zone, pigmentary anomalies, vitelliform material deposition, signs of formation of foci of geographic atrophy).
- Individualize observation intervals (depending on the type of drusen, the dynamics of their structural changes and other risk factors).
- Among the new promising methods of treating dry AMD at the drusen stage is multiwavelength photobiomodulation.
Multiwavelength photobiomodulation:
This method is aimed at stopping or regressing the progression of dry AMD by modulating mitochondrial activity and consists of the use of specific light (red and near-infrared spectrum from ~590 to 850 nm), which can reduce oxidative stress in retinal cells, inflammation and apoptosis of PES cells.
The efficacy as a potential treatment approach has remained controversial until recently: studies have shown only temporary improvement in visual function and reduction in drusen volume (not maintained for 6 months).
Updated data from the LIGHTSITE III study were presented at the ARVO 2025 conference. They showed that photobiomodulation can significantly slow the decline in visual acuity and reduce the rate of expansion of HA zones
Recently, the FDA approved photobiomodulation for the treatment of AMD.
For complications:
- Neovascular AMD– anti-VEGF.
- Geographic atrophy – injectable drugs (inhibitors of the C3 and C5 complement system), approved by the FDA
The role of AI drusen quantification OCT
The role of AI: automated drusen-volume measurement in OCT is now a reality. IT allows automated segmentation and counting (3D volume, area, height), identification of reticular pseudodruses and other signs of AMD, and compilation of prognostic profiles.
In practice, applying an OCT drusen-counting algorithm reduces variability in assessments and helps personalize visit frequency. Additionally, home OCT monitoring models with AI analysis are being developed, indicating that broader AI support for AMD is fast approaching.
Conclusion
Drusen on OCT are more than just a sign of AMD. They have become one of the most important biomarkers of age-related macular degeneration and a kind of “compass” in the daily practice of an ophthalmologist. Today we understand that:
Drusen come in different types, and, accordingly, carry different prognostic information: hard, soft, confluent, and reticular pseudodrusen. Each type carries a different risk and requires a different surveillance strategy.
Drusen levels are no longer limited to diameter, height, volume, dynamics, and structural features as well as accompanying OCT biomarkers have also become important. It is the combination of these parameters that allows us to predict the transition to the late stages of AMD.
OCT has changed the game: drusen can now be seen in 3D, segmented automatically, build PES elevation maps, and compare data between visits. Thanks to this, the doctor receives a lot of information about the evolution of the disease.
AI sets a new standard: algorithms can accurately calculate drusen volume, identify their subtypes, generate prognostic profiles, and reduce interobserver variability. This translates data from subjective descriptions into objective, reproducible numbers.
Drusen classification on OCT using AI allows not only ascertaining the presence of drusen, but also differentiating their type, objectively measuring their number and parameters, and tracking their dynamics via AI drusen quantification on OCT. For the doctor, this means identifying risk factors in the early stages of retinal disease, accurately comparing data between visits, and prescribing the correct therapy promptly.
Home monitoring is the future that has already begun: the first FDA-approved solutions with “OCT + AI” are currently used to monitor fluid in neovascular AMD, but they pave the way for daily structural monitoring of drusen as well. This means that in the near future, the patient may be able to monitor their own retina at home, and the doctor may be able to see the dynamics in real time.
In the treatment of drusen wet or dry AMD, the main goal remains not to “remove drusen,” but to minimize risks (smoking, diet, systemic factors), prescribe AREDS2-based complexes, timely detect complications, and apply already available therapies (anti-VEGF in INM, C3 and C5 inhibitors of the complement system in HA). Among the new promising methods for treating dry AMD at the drusen stage is multiwavelength photobiomodulation.
It is important to remember when communicating with the patient: drusen is not a therapeutic target, but a structural “compass”. We do not “treat drusen.” Instead, we systematically reduce risks (smoking, blood pressure, nutrition), use drugs based on the AREDS2 formula, and most importantly, we regularly measure their quantitative parameters in dynamics. When complications appear and the transition to a late stage occurs, we prescribe treatment based on the same objective OCT metrics. Thus, instrumental accuracy and AI analytics turn drusen into a manageable marker that helps to timely detect the risks of AMD progression.
Thus, drusen on OCT have become a bridge between morphology and prognosis. They provide an opportunity to build a long-term strategy for preserving vision. Today, the doctor is required not only to see drusen, but also to quantitatively measure, assess in dynamics, calculate the risk, and explain to the patient his individual risks. It is thanks to these approaches that we are moving towards a new paradigm – personalized ophthalmology, where decisions are made based on objective digital data, enhanced by artificial intelligence.
Sources:
-
- https://pubmed.ncbi.nlm.nih.gov/39558093/
- https://jamanetwork.com/journals/jamaophthalmology/fullarticle/2765650
- https://link.springer.com/article/10.1007/s00417-024-06389-x
- https://iovs.arvojournals.org/article.aspx?articleid=2804052
- https://www.ophthalmologyscience.org/article/S2666-9145(25)00182-4/fulltext
- https://www.nature.com/articles/s41433-024-03460-z
- https://www.ophthalmologytimes.com/view/arvo-2025-update-on-the-lightsite-iii-study-in-amd
-
Central Retinal Vein Occlusion CRVO OCT: Detection and Modern Approaches to Monitoring and Treatment
Maria Znamenska
3 min.Introduction
Central Retinal Vein Occlusion (CRVO) OCT is one of the most common and clinically significant vascular disorders affecting the eye, often resulting in substantial visual impairment. This condition ranks second among causes of vision loss due to vascular disease, after diabetic retinopathy, placing a considerable burden on both healthcare systems and patients’ quality of life. Epidemiological studies show that the prevalence of RVO increases with age, and in populations with concomitant cardiovascular disease, the risk of developing occlusion rises severalfold.
Despite a long history of study, it is the breakthroughs in instrumental diagnostics over the past decade that have fundamentally changed our approach to recognizing and managing RVO. Previously, assessment of the macula and retinal vasculature relied primarily on ophthalmoscopy. While still an important tool, it has inherent limitations.
Optical coherence tomography (OCT) has revolutionized diagnostic standards. With its high resolution and ability to capture subtle structural changes within the retinal layers, OCT has become indispensable for determining disease severity, monitoring treatment efficacy, and conducting long-term follow-up. It allows for the detection of minimal early signs of edema, subclinical structural damage, and initial manifestations of ischemia—changes that were practically inaccessible for dynamic assessment 10–15 years ago.
This level of precision is particularly critical for patients at increased risk of RVO. The most vulnerable groups include individuals with arterial hypertension, diabetes mellitus, glaucoma, coagulation disorders, as well as older adults, in whom the vascular walls may already have undergone degenerative or sclerotic changes.
Importantly, modern RVO treatments require objective dynamic monitoring. OCT enables precise evaluation of structural changes, tracking of therapeutic response, and individualization of treatment strategies, helping to avoid both overtreatment and undertreatment.
Thus, the role of OCT today goes far beyond simple visualization: it is a key tool for prognostic assessment, patient stratification, optimization of therapeutic decisions, and timely detection of complications.
1. What RVO Is and Why It Occurs?
Central Retinal Vein Occlusion (CRVO) OCT is a disruption of venous blood outflow in the retina due to partial or complete vein occlusion. As a result, the following occur:
- Blood stasis
- Increased venous pressure
- Impaired capillary perfusion
- Retinal edema, especially in the macular area
- Risk of neovascularization
Early detection is critical, as prompt treatment—particularly for macular edema—significantly increases the chances of preserving or restoring vision. Delayed diagnosis can lead to progression of ischemia, neovascularization, neovascular glaucoma, and persistent macular dysfunction.
RVO also has important systemic implications: patients with a history of RVO have a higher risk of acute cardiovascular events (myocardial infarction, stroke, heart failure) compared with the general population. This emphasizes the need for comprehensive management, involving not only ophthalmologists but also other specialists, such as cardiologists.
Central vs. Branch Retinal Vein Occlusion: Pathogenesis Differences
- Central Retinal Vein Occlusion (CRVO) occurs when blockage happens at the level of the lamina cribrosa. Compression, arterial wall thickening, or thrombotic processes disrupt blood outflow from the entire retina. Typical signs include:
- Diffuse hemorrhages
- Marked macular edema
- Increased risk of optic disc and iris neovascularization due to severe ischemia
- Generally worsen prognosis than branch occlusions
- Branch Retinal Vein Occlusion (BRVO) usually occurs at arteriovenous crossings, where a thickened artery compresses a vein, causing localized occlusion. Characteristic features include:
- Localized edema and hemorrhages
- Clear segmental distribution
- Prognosis is generally better than that of CRVO, though macular edema may persist
Key Risk Factors for RVO
Modern studies and guidelines identify the following as the main risk factors:
- Arterial hypertension
- Atherosclerosis and age-related vascular changes
- Diabetes mellitus (even without diabetic retinopathy)
- Glaucoma and elevated IOP
- Hypercoagulable states, thrombophilia
- Obstructive sleep apnea
- Age >50 years
Rare cases of RVO associated with thromboembolic complications after COVID‑19 infection or vaccination have also been reported, highlighting the ongoing relevance of thrombotic mechanisms.
Impact on Microcirculation and Vision
RVO leads to:
- Impaired normal venous outflow
- Sharp elevation of hydrostatic venous pressure
- Damage to the blood-retinal barrier
- Leakage of plasma and cellular elements into the retinal interstitium, causing macular edema
- Development of ischemic zones
- Over time, thinning of inner retinal layers, neuroepithelial atrophy, and damage to the photoreceptor layer
These changes are best assessed with OCT, which enables precise patient stratification and treatment planning. Timely diagnosis, proper monitoring, and early therapy are essential.
2. OCT Signs of Retinal Vein Occlusion: Detecting Subtle Changes
With the advent of OCT, detection of structural retinal changes in RVO has significantly improved—even at early stages without obvious clinical signs.
Acute Stage Changes (first weeks after occlusion)
- Macular edema:
- Cystic spaces in inner retinal layers (INL, OPL)
- Increased central retinal thickness
- Subretinal fluid (serous neurosensory detachment)
- Intraretinal hemorrhages: appear on OCT as hyperreflective areas with shadowing of underlying layers
- Ischemia indicators:
- Hyperreflectivity of neuroepithelium
- Cotton-wool spots
Chronic Stage Changes (months later)
- Chronic ischemic and atrophic changes (thinning of inner retinal layers)
- Disruption of photoreceptor layer (ELM and EZ)
- Disorganization of inner retinal layers (DRIL)
- Persistent edema (>6 months) indicates chronic RVO requiring therapeutic adjustment
AI for OCT thus allows both acute diagnosis and long-term monitoring of ischemic progression or tissue remodeling.


3. Assessment of Macular Changes in RVO Using OCT
Central retinal vein occlusion crvo OCT is now considered the gold standard for diagnosing, monitoring, and assessing treatment response in macular edema, including that associated with RVO.
OCT is highly sensitive for:
- Quantitative and qualitative analysis (central retinal thickness [CRT], macular volume [MV], size and number of cystic spaces, DRIL, photoreceptor layer integrity)
- Evaluating treatment response
- Detecting minimal residual cysts
- Predicting visual acuity outcomes
Typical OCT Findings in RVO:
- Diffuse retinal thickening
- Cystoid macular edema (localized cysts deforming normal retinal architecture)
- Serous neurosensory detachment (indicative of blood-retinal barrier breakdown)
- Disruption of EZ and ELM (photoreceptor involvement, critical for final visual acuity)
These capabilities make OCT an integral part of modern RVO monitoring.

4. Top 3 Challenges in RVO OCT Analysis
Despite its power, OCT assessment of RVO has significant limitations:
- Need for normative comparison
Interpretation requires comparison with the patient’s contralateral eye or established normal values. Systemic vascular anomalies can affect both eyes, limiting standardization. - Complexity with comorbidities
Many RVO patients have systemic (hypertension, diabetes) or ophthalmic comorbidities (diabetic retinopathy, AMD, glaucoma, epiretinal membrane), complicating interpretation. It can be difficult to distinguish RVO-related changes from combined pathology. - Requirement to consider the clinical context
OCT provides only part of the clinical picture. Accurate interpretation requires integration of symptoms, medical history, systemic factors, fundoscopic findings, and other diagnostic tests. Anatomical variations, comorbidities (glaucoma, cataract), and individual treatment response also necessitate a personalized approach.
5. Treatment of RVO: Modern Approaches
Currently, no treatment restores normal retinal venous circulation. Therefore, therapy focuses on controlling complications, primarily macular edema and preventing neovascularization (retinal, iris/optic disc, neovascular glaucoma, hemorrhages, and tractional changes).
All RVO patients should receive systemic management, ideally in collaboration between an ophthalmologist and a cardiologist or internist. Monitoring of blood pressure, lipids, glucose, and coagulation factors is essential, as RVO often signals systemic vascular risk.
Treatment decisions must be individualized, considering:
- RVO subtype (CRVO vs. BRVO)
- Edema severity
- Clinical and OCT findings
- Risk of adverse effects
- Patient status (comorbidities, ability for regular follow-up)
Anti-VEGF Therapy as First-Line Treatment
Intravitreal anti-VEGF injections are the first-line therapy for macular edema associated with RVO. These drugs reduce vascular endothelial growth factor (VEGF) expression, lowering vascular permeability, fluid leakage, edema, and inhibiting pathological neovascularization.
Commonly used agents:
- Ranibizumab, Aflibercept, Faricimab: proven safe and effective for CRVO and BRVO-related macular edema brvo vs crvo oct; studies show significant improvements in best-corrected visual acuity (BCVA) and central macular thickness (CMT).
- Bevacizumab: used off-label for macular edema and neovascularization.
Long-term studies indicate anti-VEGF therapy provides sustained visual improvement for many patients, with injection frequency often decreasing over time.
Advantages:
- High efficacy for macular edema
- Good tolerability and safety (systemic complications are rare)
- Personalized treatment possible
Limitations / Challenges:
- Some patients respond insufficiently
- Requires frequent injections (clinic visits, financial burden, potential complications, patient discomfort)
- Chronic or refractory edema may require alternative or combination approaches
Steroid Implants and Injections: Second-Line Therapy
Dexamethasone intravitreal implant (OZURDEX) is approved for RVO-related macular edema, particularly when:
- Anti-VEGF therapy is insufficient
- Frequent injections are impractical (distance, transportation, cost)
Steroids reduce inflammation, vascular permeability, and fluid accumulation, useful in chronic or resistant edema.
Risks / Limitations:
- Cataract (especially with repeated or long-term use)
- Increased intraocular pressure (IOP), potential steroid-induced glaucoma
Laser Therapy
- Panretinal photocoagulation is effective for neovascularization.
- Its use has declined with anti-VEGF availability, which offers strong anatomical and functional results.
Surgical Approaches
- Vitrectomy may be considered in selected cases.
- Surgery carries risks and is reserved for situations where other treatments fail or are inappropriate.
Combination Strategies
- In practice, clinicians often combine anti-VEGF therapy with steroid implants or laser treatment, depending on disease course.
- This can reduce total injection burden, minimize side effects, and improve outcomes in chronic or recurrent edema.
Monitoring Frequency
- Active macular edema or ongoing treatment requires regular OCT follow-up to evaluate therapeutic response and adjust injection intervals.
- OCT schedule:
- Monthly at treatment initiation
- Individualized intervals using Treat-and-Extend protocols
- Structural monitoring to prevent atrophic changes
- Ischemic RVO patients have the highest neovascularization risk within the first 90 days; monthly monitoring during the first 6 months is critical.
Conclusions and Recommendations
RVO is a complex, multifactorial vascular disorder that can cause sudden and severe vision loss, particularly in patients with systemic risk factors. Modern management aims not only to address acute complications but also to control long-term structural retinal changes.
OCT has transformed RVO care by providing:
- Early detection of edema, subclinical ischemia, and architectural changes
- Dynamic monitoring of treatment response, allowing timely adjustments and optimization
- Improved long-term prognostication through evaluation of macular thickness, outer retinal layers, and fluid volume
OCT helps identify edema type and secondary changes—atrophy, photoreceptor damage, inner retinal thinning—allowing a more accurate visual prognosis, especially in ischemic RVO.
When combined with modern anti-VEGF agents, long-acting steroid implants, and personalized dosing regimens, OCT enables:
- Reduction of unnecessary injections via interval optimization
- Maximized treatment efficacy based on morphological findings
- Prevention of recurrence and progression through early detection of edema
Thus, OCT is not merely a visualization tool but a core element of clinical decision-making, improving patient management, preventing complications, and enabling more complete and stable visual recovery.
Clinical Recommendation: Integrate regular OCT assessments into RVO management, with attention to macular thickness dynamics and outer retinal layer integrity for precise disease control and optimized therapeutic outcomes.
References:
- https://pubmed.ncbi.nlm.nih.gov/38714470/
- https://www.rcophth.ac.uk/wp-content/uploads/2015/07/Retinal-Vein-Occlusion-Guidelines-Executive-Summary-2022.pdf
- https://www.mdpi.com/2077-0383/14/4/1183
- https://www.auctoresonline.org/article/clinical-therapeutic-orientation-in-retinal-venous-obstruction
- https://www.mdpi.com/2077-0383/10/3/405
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10801953
- https://www.mdpi.com/2075-4418/13/19/3100
- https://karger.com/oph/article-abstract/242/1/8/255831/Microvascular-Retinal-and-Choroidal-Changes-in?redirectedFrom=fulltext
- https://link.springer.com/article/10.1007/s40123-024-01077-9
- https://pubmed.ncbi.nlm.nih.gov/39717563/
- https://provider-rvo.vision-relief.com/introduction/management/
-
Key Trends in Ophthalmology and Optometry in 2026
Maria Znamenska
3 min.Introduction
The year 2026 in ophthalmology will not be defined by a single “major breakthrough,” but rather by key trends in Ophthalmology and optometry in 2026, and the maturation of several directions whose discoveries and innovations are now transitioning into everyday clinical practice. While just a few years ago innovations were often perceived as isolated technologies far removed from real-world care (a new drug, device, or piece of equipment), today entire ecosystems are being formed: from early detection to long-term monitoring, from the ophthalmologist’s office to optometric screening, from a single consultation to a longitudinal patient journey supported by digital tools.
The core logic of 2026 is a shift from reactive to proactive ophthalmology. Increasingly, the goal is to prevent disease at the stage of risk-factor modification, intervene in the earliest pathological changes, and track preclinical markers. This shift is visible across several dimensions: the growing role of telemedicine and portable diagnostics; autonomous AI becoming a public health tool; and oculomics, which enables ocular image analysis to serve as a source of early biomarkers for systemic conditions. At the same time, the treatment paradigm is evolving: where repeated procedures once dominated (for example, frequent intravitreal injections), 2026 brings a move toward extended-duration regimens, implant-based drug delivery platforms, and disease control with fewer clinic visits.
Another important axis is the alignment of patient expectations. Some new approaches (for example, in the management of dry AMD and geographic atrophy) do not promise to “restore vision,” but rather to buy time—slowing structural retinal damage and functional vision loss. As a result, in 2026, risk–benefit communication and shared decision-making become almost as important as the choice of molecule or device itself.
Below, we outline the key eye care trends of 2026: what is changing, why it matters, and how it will shape ophthalmic and optometric practice.
1. New Approaches to Treatment
1.1. Geographic Atrophy (GA): The Introduction of Active Treatment in eye care trends 2026
1.1.1. Injectable Therapies as Ophthalmology Trends 2026
Following the key trends in Ophthalmology and Optometry in 2026 , development of injectable therapies for geographic atrophy, clinical practice is entering a “second wave” phase—where the main questions are no longer whether therapy is possible for a disease historically considered untreatable, but how that therapy should be practically implemented. In 2026, the focus will be on patient selection, treatment initiation, dosing frequency and duration, as well as monitoring.
Currently, the FDA has approved the following injectable therapies for GA:
- Izervay (avacincaptad pegol) — a C5 complement inhibitor.
- Syfovre (pegcetacoplan) — a C3 complement inhibitor.
Their mechanism of action involves reducing chronic inflammation and cellular damage in the retina and—most importantly—slowing the rate of GA lesion expansion.
Because most available data focus on slowing atrophy progression (an anatomical endpoint) rather than guaranteed improvements in visual acuity, properly managing patient expectations becomes particularly critical in 2026. Clear discussions about therapeutic goals and limitations are emphasized in review publications addressing the first approved GA treatments.
1.1.2. Multiwavelength Photobiomodulation
Multiwavelength photobiomodulation is one of the most promising emerging approaches and key trends in Ophthalmology and Optometry in 2026 aimed at halting or slowing the progression of dry AMD through modulation of mitochondrial activity. The use of specific wavelengths (red and near-infrared light, approximately 590–850 nm) may reduce oxidative stress in retinal cells, inflammation, and apoptosis of retinal pigment epithelium cells.
Its appeal is clear: a non-invasive procedure with significantly better acceptability for some patients compared with regular injections.
Until recently, its effectiveness remained debated, with studies showing only temporary functional improvement and reduction in drusen volume. At ARVO 2025, updated results from the LIGHTSITE III study demonstrated that photobiomodulation can significantly slow visual acuity decline and reduce the rate of GA expansion.
In 2025, the FDA approved photobiomodulation for AMD, creating strong prospects for broader clinical adoption in 2026.
The 2026 trend is correct positioning and stratification:
- Use of photobiomodulation based on clear indications for specific dry AMD stages and patient profiles.
- Transparent communication of expectations, with goals focused on functional support and slowing GA progression rather than guaranteed vision restoration.
1.2. Extended Anti-VEGF Treatment Regimens
Another major trend is the shift toward regimens with reduced injection frequency. This is not merely about comfort, but primarily about preventing missed visits: patients with AMD and diabetic retinopathy with DME often fall out of treatment due to visit burden. Thus, 2026 reinforces the principle that treatment must be effective in real-world conditions, not only under ideal adherence.
The ranibizumab port delivery system (Susvimo, Port Delivery System) has become emblematic of this trend. In 2025, the FDA also approved Susvimo for the treatment of diabetic retinopathy.
1.3. Gene Therapy for Macular Telangiectasia Type 2 (MacTel 2)
MacTel 2 is a chronic, progressive neurodegenerative retinal disease that previously lacked active treatment.
In 2025, the first implantation of ENCELTO (revakinagene taroretcel)—the first and currently only FDA-approved gene therapy for MacTel 2—was performed in the United States. ENCELTO enables a shift from observation to active intervention, with the potential to preserve visual function in early-stage patients.
The device is based on encapsulated cell therapy technology: a capsule containing genetically modified cells that continuously secrete recombinant human ciliary neurotrophic factor (CNTF), acting as a neuroprotective agent that slows photoreceptor degeneration.
In 2026, the focus will move from “innovation storytelling” to routine clinical implementation, including defining early selection criteria, monitoring protocols (OCT biomarkers, functional testing), and accumulating real-world long-term data on photoreceptor preservation and visual function.
1.4. Gene Therapy for Neovascular AMD: Closest to Real Transformation
For neovascular AMD, gene therapy remains one of the most anticipated eye care trends 2026 directions, as it has the potential to fundamentally change treatment logic—from repeated injections to a single vector administration enabling long-term therapeutic protein expression. Reviews published in 2025 highlight active programs such as RGX-314, ADVM-022 (Ixo-vec), 4D-150, and others.
In 2026, the key questions shift from “does it work?” to “how does it work across different patient groups?” including:
- Stability and duration of expression;
- Inflammatory and immune response profiles;
- Need for supplemental anti-VEGF therapy;
- Patient selection criteria;
Injection centers and post-procedure monitoring standards.
2. Oculomics: The Eye as a “Window to the Body” and a Source of Digital Biomarkers
Oculomics is one of the most compelling trends of 2026, as it reshapes ophthalmology’s role within medicine as a whole. The concept is simple: the eye is the only structure where microvasculature, neurons, and signs of metabolic and inflammatory processes can be visualized non-invasively at high resolution. As a result, fundus and OCT/OCTA data may serve as biomarkers for systemic conditions—from cardiovascular risk to neurodegenerative diseases.
In contemporary research, oculomics is described as an approach that uses retinal images to assess systemic risks and conditions, with potential scalability for screening. In 2026, this “scale” becomes critical: data may originate not only from ophthalmology clinics, but also from optometric practices, mobile screening programs, and telemedicine.
What truly changes in 2026:
- A transition from “interesting correlations” to clinical utility, with models expected to demonstrate actionable impact on patient management.
- Data verification and management of false-positive risk, including the communication of systemic risk to patients.
- Integration with AI, as multidimensional patterns often exceed human interpretive capacity.
A major risk in 2026 is over-marketing, reinforcing the need for externally validated models with clear clinical context that do not generate unnecessary “medical noise.”
3. AI Technologies: From Decision Support to Autonomous Screening and Managed Patient Pathways
3.1. Autonomous Diabetic Retinopathy Screening as a Scalable Standard
In 2026, diabetic retinopathy remains the most studied use case for autonomous AI. In the United States, three FDA-approved autonomous DR screening systems are already described (LumineticsCore/IDx-DR, EyeArt, AEYE-DS). This positions AI as a practical tool capable of influencing large-scale screening programs, particularly in primary care, endocrinology clinics, and mobile settings.
The FDA approval of AEYE-DS as a fully autonomous solution (portable camera plus algorithm) underscores that in 2026, AI increasingly “works where the patient is,” not only where an ophthalmologist is present.
3.2. 2026 as the Year of Integration
Successful projects in 2026 will be distinguished by:
- Image quality standards and quality control;
- Clear referral rules and urgency levels;
- Mechanisms to ensure patient follow-through (scheduling, reminders, visit tracking);
- Transparent documentation for clinicians, patients, and audit purposes.
3.3. AI as “Invisible Infrastructure”
In 2026, AI increasingly functions as invisible infrastructure: highlighting high-risk cases, prioritizing queues, generating structured reports, and standardizing interpretation. The impact is reduced variability, faster routing, and fewer missed cases.
4. Telemedicine: From Video Calls to Retinal Screening and Remote Management
By 2026, telemedicine in ophthalmology is no longer synonymous with video consultations. Its foundation is tele-imaging: transmission and assessment of retinal images (fundus photos, sometimes OCT) with structured referral protocols.
At the same time, limitations become more openly discussed. Certain conditions and components of assessment may be less accurately captured remotely, requiring clear protocols to define which patients can be managed remotely and which require in-person examination.
The 2026 trend is a shift from “tool” to “pathway”:
- Tele-screening as the first step;
- Automated or semi-automated reporting;
- Referral and follow-up control;
Remote reassessment for ongoing risk monitoring.
5. New Devices and Portable Diagnostics: Closer, Faster, More Scalable Care
5.1. Portable Diagnostics as the Foundation of Coverage
Portable fundus cameras and compact diagnostic systems represent one of the most practical changes of 2026. Their value lies not only in technology, but in enabling large-scale screening in locations without full ophthalmic infrastructure.
Synergy with autonomous AI (such as AEYE-DS) is especially strong here, supporting new partnership models:
- Endocrinology and primary care clinics;
- Optical stores and optometric practices;
- Mobile programs for workplaces or regions.
5.2. Devices Deliver Value Only with Quality Protocols
Success depends not just on acquiring devices, but on defined protocols:
- Staff training in image acquisition;
- Minimum quality criteria;
- Retake rules;
- Handling ungradable cases.
In 2026, image quality becomes decisive, as AI and telemedicine depend on it.
5.3. Home and Remote Monitoring for Extended Treatment Regimens as eye care trends 2026
As treatment intervals lengthen, the risk of between-visit deterioration increases. Thus, 2026 strengthens the role of:
- Home functional monitoring;
- Digital questionnaires and symptom trackers;
Remote checkpoints signaling the need for earlier recall.
6. 2026 as the Year of Standardized Myopia Control and Greater Risk Awareness
By 2026, myopia control is no longer debated but formalized, grounded in consensus documents and systematic reviews. Myopia is increasingly recognized as a chronic disease with stages, phenotypes, and potentially blinding complications.
Implications for practice:
- Focus on preventing progression to high myopia.
- Combined strategies integrating behavioral, optical, and pharmacologic interventions with monitoring.
- A shared language between optometrists and ophthalmologists, with coordinated patient pathways.
- Support from AI and telemedicine for risk detection and personalized care.
Myopia control in 2026 becomes a structured, long-term risk-reduction process.
7. Optogenetics: Expanding the Evidence Horizon in Inherited Retinal Degenerations
In 2026, optogenetics moves beyond concept into longer-term observation. Publications from 2025 highlight functional stabilization or improvement in retinitis pigmentosa, emphasizing pragmatic success criteria.
For patients with severe vision loss, meaningful outcomes extend beyond visual acuity charts to spatial orientation, object recognition, and contrast sensitivity. In 2026, discussions increasingly focus on realistic endpoints and honest communication of limitations.
8. Less Invasive Interventions and Patient Comfort as Components of Clinical Effectiveness
Another key eye care trends 2026 is less traumatic technology that preserves efficacy while improving patient experience. A notable example is the FDA approval of Epioxa (epi-on) for keratoconus in 2025, preserving corneal epithelium and potentially reducing pain and recovery time.
This trend spans refractive surgery, ocular surface disease, and chronic condition management, reinforcing that patient experience is integral to adherence and clinical outcomes.
Conclusion
The ophthalmology trends 2026 clearly demonstrate that ophthalmology and optometry are entering a phase of mature transformation, where success is driven not by isolated innovations but by their integration into coherent clinical pathways. The focus is shifting from treating consequences to early detection, slowing progression, and long-term management of chronic eye disease.
Active treatment of geographic atrophy, photobiomodulation, extended anti-VEGF regimens, and the emergence of gene therapies for MacTel 2 and neovascular AMD fundamentally reshape patient management—from observation or frequent procedures to strategies aimed at preserving retinal structure and function with minimal procedural burden. These approaches require careful patient stratification and responsible expectation management, as the goal increasingly becomes slowing neurodegeneration rather than restoring vision.
At the diagnostic level, 2026 reinforces decentralization: portable devices, telemedicine, and autonomous AI bring screening closer to patients and enable coverage of much broader populations. Oculomics and AI transform ocular images into sources of digital biomarkers that may influence not only ophthalmic but also general clinical management. At the same time, it becomes clear that technological value is defined not by algorithms or devices, but by data quality, model validation, and clearly structured patient pathways—from screening to treatment.
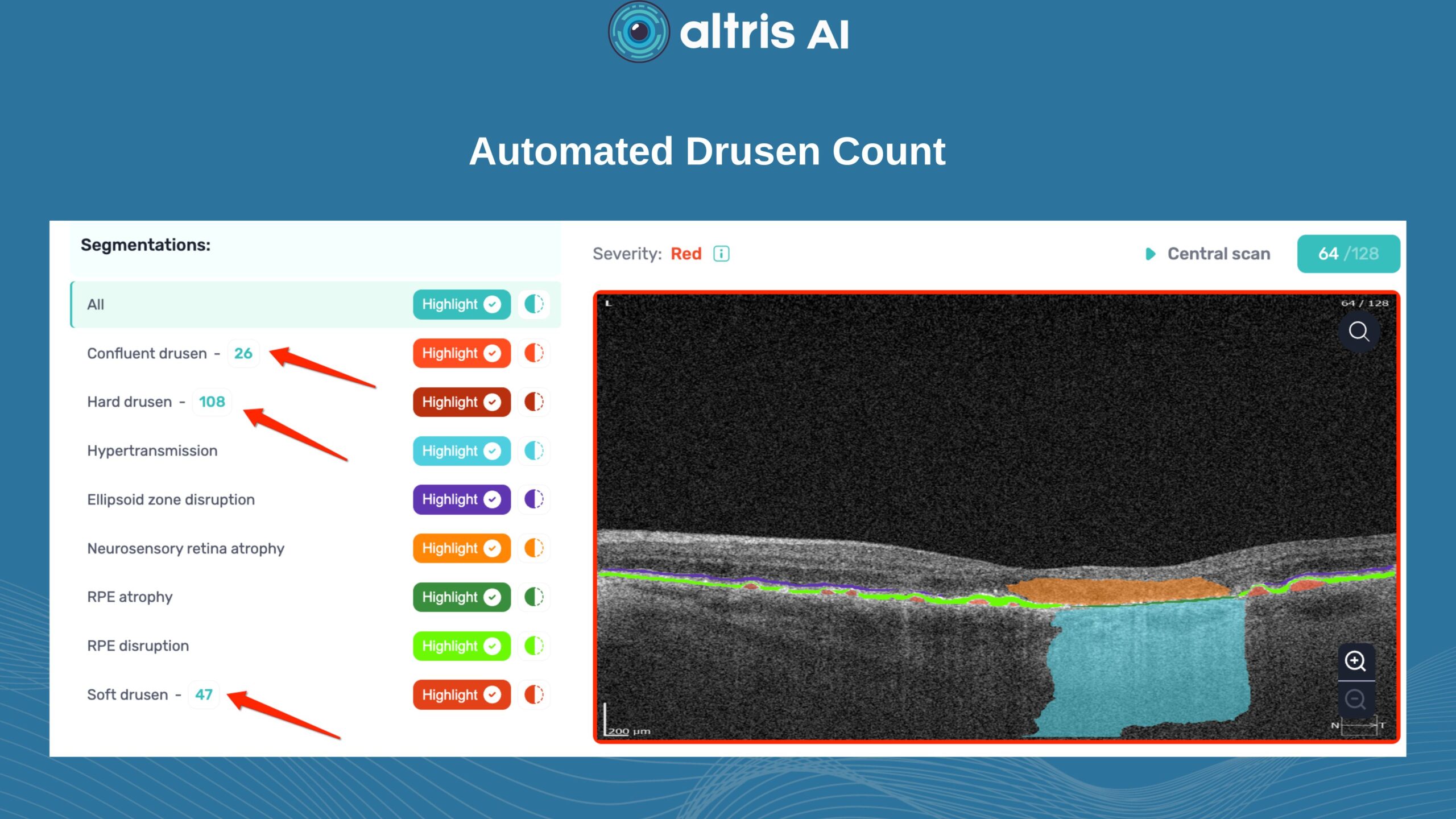
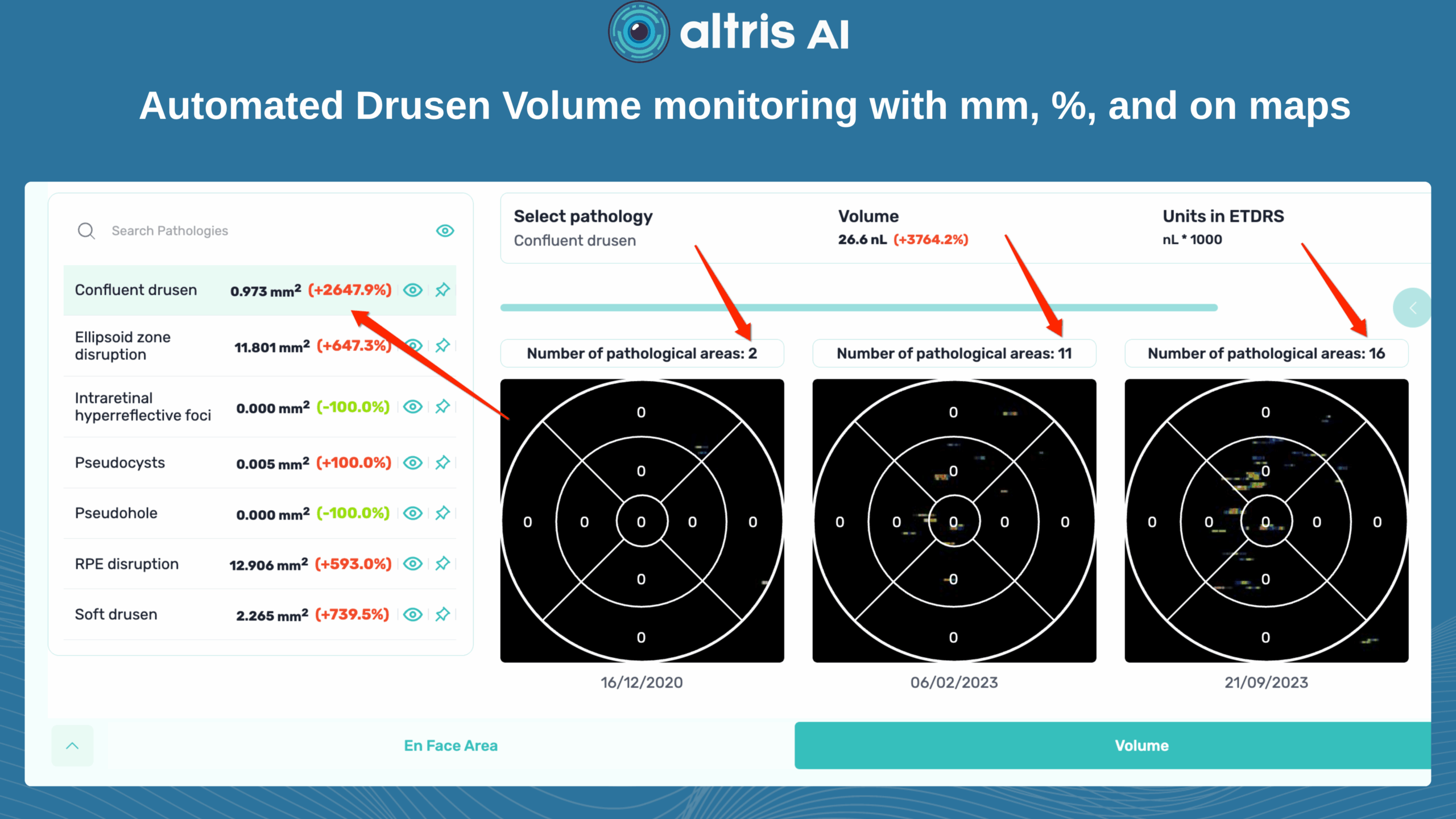
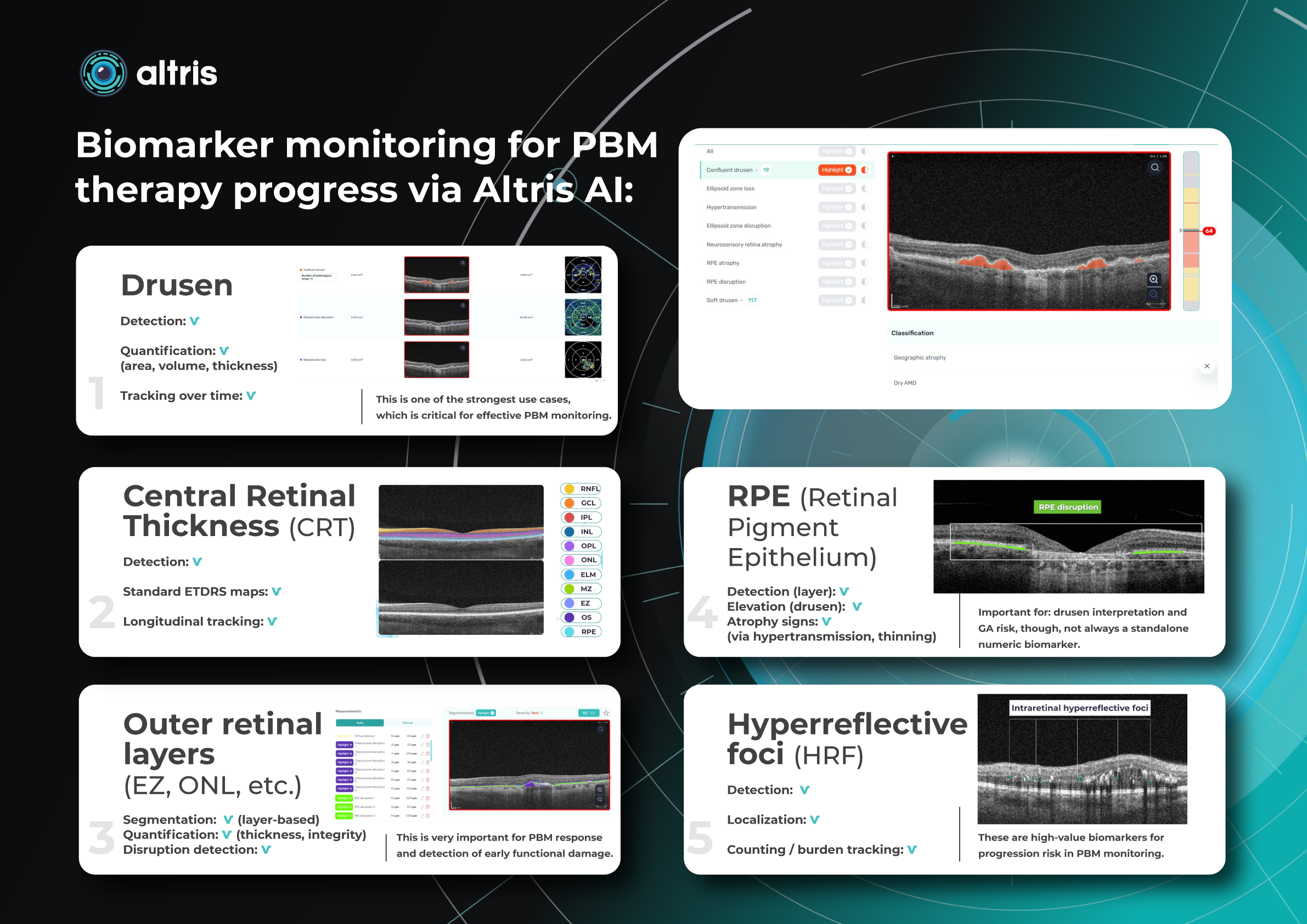
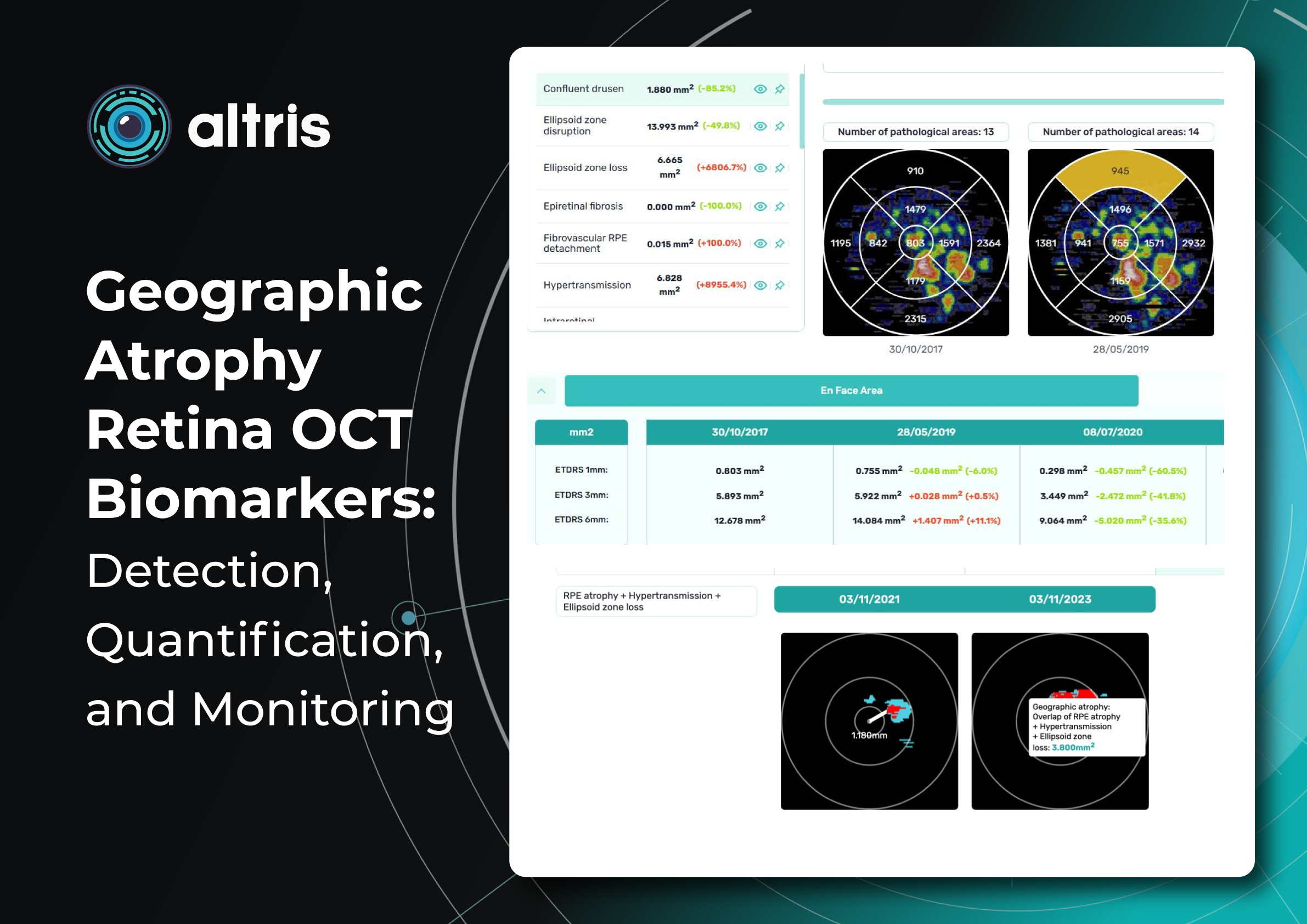
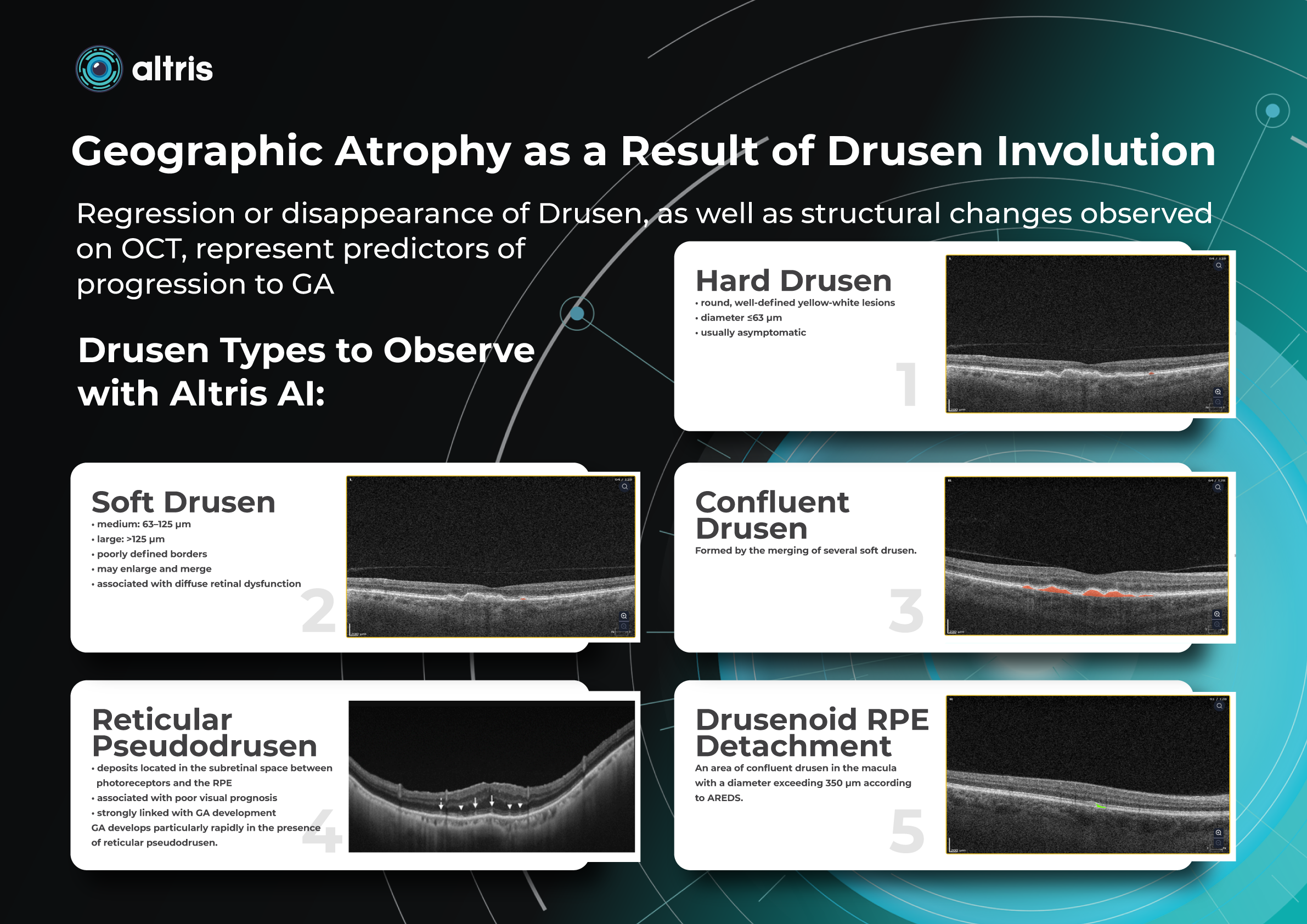
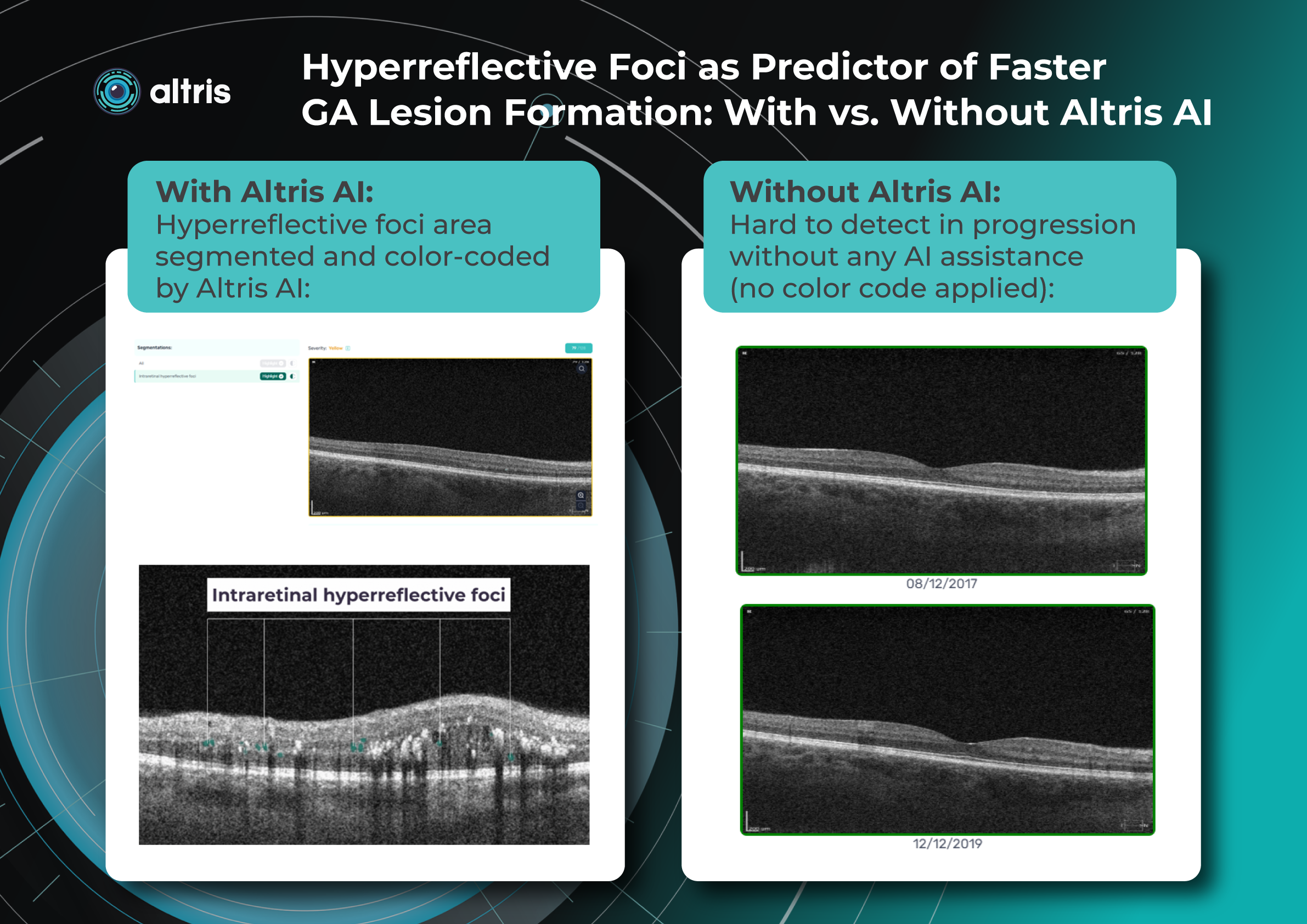
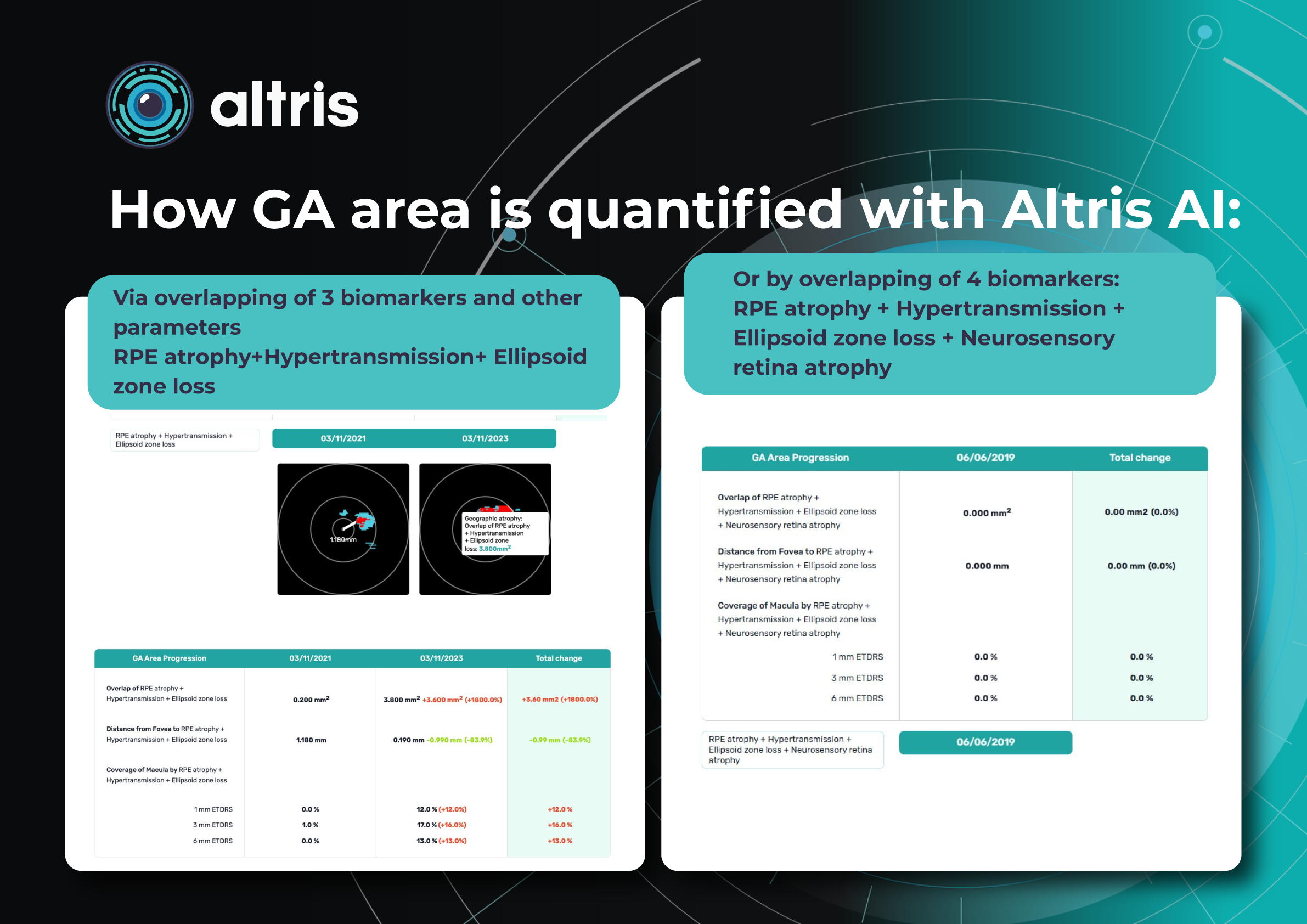







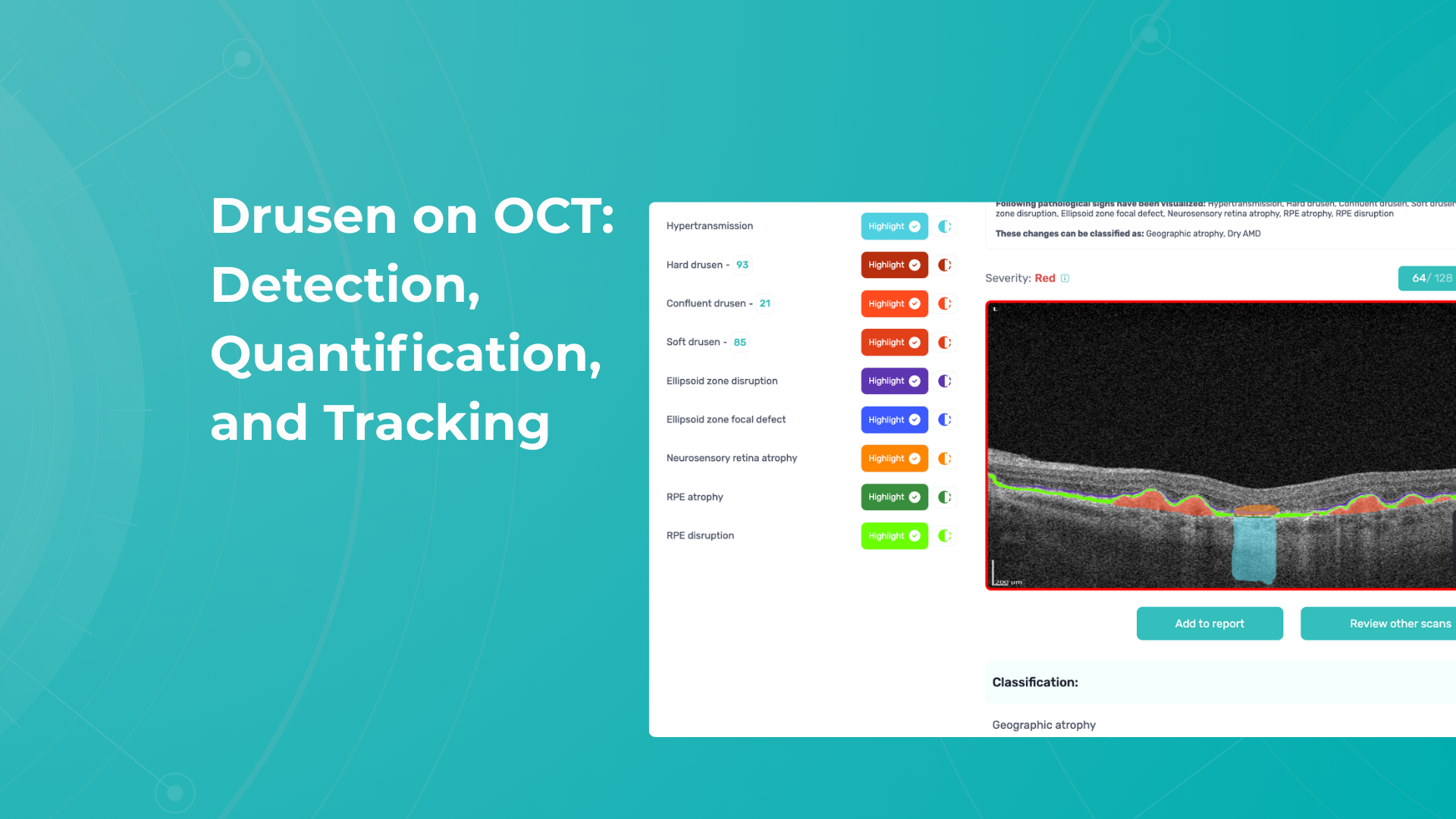






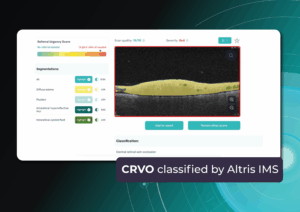
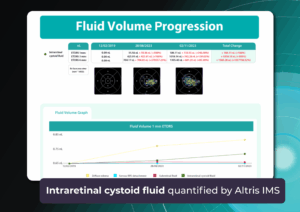
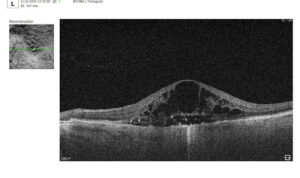


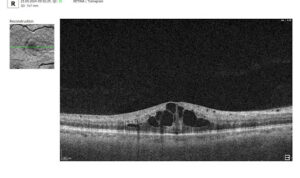
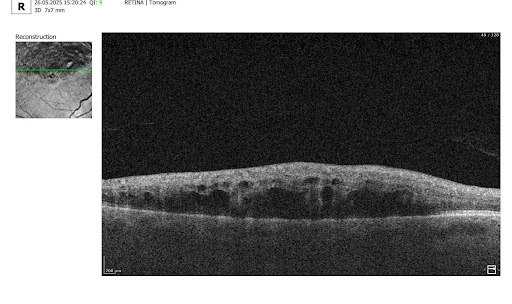







Recently Posted
-

Altris Introduces Next-Generation Fluids and GA Quantification Features
Maria Znamenska, MD, PhD Ophthalmology
1 min. readAltris Introduces Next-Generation Fluids and GA Quantification Features
Altris AI, a pioneering force in artificial intelligence for OCT scan analysis, has unveiled additional quantification features for Fluids and Geographic Atrophy (GA) tracking on its web platform. Altris AI currently detects over 70 retina pathologies and biomarkers. However, we have decided to enhance its capabilities by adding additional Fluids and GA quantification and tracking functionalities, recognizing that eye care specialists frequently work with these conditions.
These advancements empower eye care professionals (ECPs) with cutting-edge tools for diagnosing and managing retinal diseases. By integrating AI-driven quantitative tracking and progression monitoring, Altris AI enables specialists to deliver more personalized and effective treatments, ultimately enhancing patient outcomes.
Fluids Quantification and Progression Tracking
The presence of fluids such as Intraretinal Cystoid Fluid (IRC), Diffuse Edema, Subretinal Fluid (SRF), and Serous Retinal Pigment Epithelium (RPE) Detachment are critical biomarkers for conditions like nAMD, DME, DR, and RVO. Accurate detection, quantification, and tracking of these fluids are essential for monitoring disease activity, evaluating treatment efficacy, and making informed prognoses.
We created specialized more detailed functions which detect these biomarkers for more specific and accurate tracking. The AI algorithm was additionally trained to work directly with fluids taking into account the importance of these biomarkers for accurate diagnostics.
Altris AI’s advanced algorithms, trained on millions of OCT scans, provide precise and objective fluid analysis. Each of the four fluid types is localized and color-coded for clarity. Quantitative metrics such as volume, area, and ETDRS grids (1, 3, and 6 mm) are calculated and presented in mm3 or nanoliters for comprehensive evaluation. The Progression Tracking feature offers historical trend analysis with intuitive visualizations through graphs and percentages. For instance, if Cystoid Fluid (IRC) increases in volume, ECPs can immediately identify and address the change.
Precision in Geographic Atrophy (GA) Monitoring
Recent advancements in GA treatment have led to a growing need for large-scale screening in clinical practice. However, this increased demand often means higher workloads and less time for in-depth analysis.
The platform facilitates automated detection, quantification, and tracking of GA by analyzing key biomarkers: Pigment Epithelium (RPE) atrophy, Hypertransmission, Neurosensory Retina Atrophy, and Ellipsoid Zone (EZ) disruption. These biomarkers are color-coded for easier identification.
We assess GA using three key criteria:
- Overlapping region of 3 biomarkers: Hypertransmission, RPE Atrophy, and Neurosensory Retina Atrophy (referred as the GA zone).
- The shortest distance from the Fovea center to the GA zone.
- Percentage of the GA zone covering the 1 mm, 3 mm, and 6 mm ETDRS grid areas.
We also improved the accuracy of a critical step in our AI pipeline: the fovea and central scan detection. Altris AI’s updated model is much more robust in detecting fovea zone and central scan now. Especially in cases when the center cannot be distinguished due to pathology presence or other reasons, the model is trained to analyze the whole surface and find reference locations from which a central scan could be determined. The new model can find an accurate center in 95% of cases, in other situations, it can efficiently estimate the center location (as opposed to a simple analysis flow used by ECPs where the geometrical center is selected). This advancement significantly enhances the precision of GA detection.
Further Progression Tracking enhances GA management by visualizing changes over time, supporting timely and accurate treatment decisions. By streamlining workflows and providing actionable insights, this feature helps ECPs make informed choices and potentially preserve vision in GA patients.
Dr. Maria Znamenska, MD, PhD, and a Chief Medical Officer at Altris AI, commented:
“We listened to our clients and introduced Fluids and GA tracking features. In 2025, eye care specialists will have the tools to combine their expertise with next-generation AI technology to effectively tackle conditions that threaten vision. Our formula is simple: detect, quantify, and track fluids, GA, and 70+ retina pathologies and biomarkers for better patient outcomes.”
About Altris AI
Altris AI is an artificial intelligence platform for OCT analysis that detects the widest range of retina pathologies and biomarkers on the market – more than 70. Leading the way in AI innovation, Altris AI provides transformative solutions that enhance the decision-making, treatment, and monitoring of retinal diseases, enabling eye care professionals to deliver exceptional patient care.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.
-
OCT Scan Normal Eye vs 8 Most Common Pathologies
Maria Znamenska
31.10.202414 min readOCT Scan Normal Eye vs. 8 Most Common Pathologies
Differentiating between an OCT scan of a normal eye vs. a pathological one is a practical skill gained after years and years of practice. However, educating yourself on the basic differences will speed up the process. Understanding the “why” and “how” behind any changes on the OCT scan, compared to a normal macula OCT, will speed up your learning curve and deepen your expertise as a retinal expert.
The article’s first part focuses on key OCT features and their meaning as a structural change for retinal architecture. The second part discusses the most recognizable OCT features of eight common pathologies.
OCT Scan: Normal Eye
When evaluating an OCT scan, the most logical step is to understand how a normal macula OCT should look. The most telling feature across all scans is the contrast between light and dark areas. Typically, the nerve fiber layer and the underlying ganglion cell layer appear brighter than the densely packed nuclear layers. This is followed by the inner plexiform layer interface, which presents as a bright, hyperreflective area.
The inner nuclear layer, composed of densely packed nuclei, appears dark. This is followed by the outer plexiform layer, the outer nuclear layer, and Henle’s layer. The external limiting membrane, an important landmark for assessing retinal health, is also visible. The ellipsoid zone (EZ) is another bright layer, while the interdigitation zone may not always be distinguishable from the underlying RPE layer, even in healthy eyes. Finally, the RPE and inner choroid appear hyperreflective.
Structure
The ELM and EZ are critical structures to assess. In a normal macula OCT, the distance between the EZ and ELM is shorter than between the EZ and the RPE. The apparent “elevation” of the EZ in the foveal center results from the elongated outer segments of the foveal cones.
It’s important to remember that not all retinal structures are readily visible on a normal macula OCT. For example, Henle’s fiber layer is more easily distinguished in the presence of retinal pathology, such as swelling or thinning. Similarly, Bruch’s membrane is usually not visualized unless there is a separation between the RPE and Bruch’s membrane, often indicative of disease.
Thickness
Choroidal thickness is another key factor in OCT assessment. A general rule of thumb is that the choroid (between the RPE and the outer choroidal boundary) is approximately as thick as the retina. Thinning of the choroid may be observed in myopic or older patients, while marked choroidal thickening can raise suspicion for diseases like central serous retinopathy.
The OCT scan also provides information about laterality. The nerve fiber layer is characteristically thicker near the optic nerve head. Conversely, if the nerve fiber layer is not visualized in its expected location on an otherwise OCT normal scan, it could signal significant nerve fiber layer loss, potentially due to glaucoma or other optic neuropathies.
Reflectivity
Specific OCT terminology helps describe scans and differentiate normal findings from pathology.
Two fundamental concepts in OCT interpretation are hyporeflectivity and hyperreflectivity, which form the basis for understanding the structural composition of the retina as visualized in an OCT scan.
Hyporeflectivity refers to the increased light transmission capacity of a structure. The OCT scanning laser beam passes through hyporeflective structures with minimal reflection. The quintessential example of a hyporeflective structure is the vitreous humor. It appears as a dark area in the uppermost portion of a normal OCT scan, situated above the retina.
But hyporeflectivity can also be pathological, deviating from the patterns observed in a normal macula OCT; in the retina, it manifests in three primary ways.
Like the vitreous, subretinal fluid exhibits high light transmission and appears black on OCT. A uniformly black region suggests the fluid lacks cellular debris or other inclusions.
Subretinal fluid on OCT
Fluid can also accumulate within the retinal layers, for example, between the layers of the neuroepithelium. This intraretinal fluid also appears hyporeflective on OCT.
Intraretinal fluid on OCT
Following a degenerative process within the retina, a cavity or void may form where retinal tissue has been lost. These degenerative cavities lack the cellular components necessary to reflect light and thus appear as dark spaces on OCT. It’s important to differentiate these cavities from cystic spaces, which may have distinct clinical implications.
One example is outer retinal tubulations. While associated with various diseases, outer retinal tubulations (ORTs) generally indicate outer retinal degeneration and atrophy.

Outer retinal tubulations on OCT
Hyperreflectivity, unlike hyporeflectivity, indicates structures with high light reflectance. On the grayscale spectrum of an OCT image, hyperreflective structures appear progressively whiter.
The retinal pigment epithelium (RPE) complex and Bruch’s membrane are considered the most hyperreflective structures in a normal macula OCT.
Pathological processes can introduce new hyperreflective elements within the retina, aiding in differentiating normal and abnormal OCT scans. A typical example is hard exudates, frequently observed in diabetic retinopathy. These lipid-rich deposits are extremely dense, causing them to appear bright white on OCT due to the complete reflection of incident light. Furthermore, this high density leads to a shadowing effect beneath the deposits, caused by strong backscattering of the OCT signal.
Hard exudates and shadowing on OCT
Epiretinal membranes (ERMs) – a thin membrane or layer of scar tissue that forms over the retina – are also hyperreflective. It is composed of dense connective tissue with high light-reflecting properties and appears white on OCT scans.
Integrity
Beyond hypo- and hyperreflectivity, OCT interpretation involves assessing the structural integrity of retinal layers. For instance, in an OCT scan of a normal eye, Bruch’s membrane appears as a thin, continuous line underlying the retinal pigment epithelium (RPE). The RPE is a monolayer of cells, ideally presenting with a smooth and uniform optical density. However, some pathologies, particularly early stages of age-related macular degeneration (AMD), may show unevenness or integrity loss in the RPE and Bruch’s membrane complex.
Disruption of the ellipsoid zone (EZ) is a particularly concerning finding on OCT, often indicating photoreceptor damage. Significant disruption of the EZ in the central macula is a strong biomarker for adverse visual outcomes.
The closer the loss of integrity extends toward the foveal center, the poorer the visual prognosis tends to be.
Ellipsoid zone disruption on OCT
OCT also plays a crucial role in visualizing and characterizing breaks in the structural integrity of the retina. These breaks, commonly referred to as retinal tears or holes, can be classified as full-thickness or partial-thickness, depending on the extent of retinal involvement.
Full-thickness breaks completely separate all retinal layers, while partial-thickness breaks involve only some retinal layers. OCT allows for precise delineation of the layers involved and the overall morphology of the break.
Retinal holes can also be categorized by their location. Macular holes, as the name suggests, involve the central retina and can lead to significant central vision loss and require prompt attention.
Lamellar macular hole on OCT
Non-macular holes occur outside the central macular region, often in the peripheral retina. While they may not cause immediate central vision disturbances, they can still lead to serious complications, such as retinal detachment, if left untreated.
Definition
The blurring of retinal structures, or loss of definition, is another key OCT concept. This loss of the retina’s normal layered organization, seen in diseases like AMD, manifests as indistinct layers merging into a homogenous mass.
Disorganisation of retinal inner layers on OCT
Hypertransmission in OCT refers to enhanced signal penetration due to reduced blockage of the OCT light signal. This phenomenon is frequently observed in geographic atrophy, a late stage of AMD characterized by the atrophy of the retinal pigment epithelium, choriocapillaris, and photoreceptors.
Hypertransmission on OCTIn a normal macula OCT, a signal is attenuated as it traverses the various retinal layers, with a portion of the signal being reflected to the detector. However, in geographic atrophy (GA), the loss of RPE and other retinal structures reduces this attenuation, allowing the OCT signal to penetrate deeper into the choroid. This increased penetration results in a stronger signal return from the choroidal layers, creating essentially a “corridor” of enhanced signal penetration through the atrophic areas of the retina. This deep penetration and strong signal return, unfortunately, indicate significant retinal damage and are associated with a poor visual prognosis.
Displacement
Another term used to describe OCT scan results is elevation. It refers to the upward displacement of retinal structures from their normal anatomical position. In the context of age-related macular degeneration (AMD), elevation is frequently associated with the presence of drusen.
Drusen are extracellular deposits that accumulate between the retinal pigment epithelium (RPE) and Bruch’s membrane. They are a hallmark of AMD and can vary in size, shape, and composition. Drusen are typically categorized as hard, soft, or confluent based on their ophthalmoscopic appearance.
Hard and soft drusen on OCT
In contrast to elevation, depression in OCT describes the inward displacement or concavity of retinal structures. This can be a manifestation of various pathological processes, with a prominent example of degenerative myopia.
Degenerative myopia on OCT
OCT scan: normal eye transformation through pathologies
Age-related macular degeneration (AMD)
AMD is an acquired degenerative macular disease usually affecting individuals over the age of 55 years. It is characterized by pathologic alterations of the outer retina, retinal pigment epithelium (RPE), Bruch’s membrane, and choriocapillaris complex, including drusen formation and pigmentary changes.
AMD is a progressive disease, and in advanced stages, central geographic atrophy and neovascularization, may develop and reduce vision. OCT plays a critical role in distinguishing between the different stages and forms of AMD, particularly when compared to the features of an OCT normal scan.
Wet AMD
Neovascular or “wet” age-related macular degeneration (nAMD) arises from the aberrant growth of choroidal vessels that penetrate Bruch’s membrane and invade the subretinal space. These abnormal vessels leak fluid and blood, disrupting the retinal architecture and causing vision loss.
Several key OCT features can signal the presence and activity of nAMD in comparison to a normal OCT scan:
- Fluid Accumulation: The presence and location of fluid are hallmarks of nAMD (hence the term ‘wet AMD’). Intraretinal fluid, appearing within the retinal layers, often signifies more severe disease and a poorer visual prognosis than subretinal fluid, which accumulates beneath the retina.
- RPE Detachment: Serous PED appears as a dome-shaped elevation of the RPE due to fluid accumulation beneath it. PEDs often accompany nAMD and can vary in size and shape.
- Disruption of Retinal Layers: nAMD can disrupt the normal retinal architecture, particularly the photoreceptor layer. Damage to the ellipsoid zone (EZ) and external limiting membrane (ELM) is visible on OCT and correlates with visual impairment.
- Hyperreflective Foci: Hyperreflective dots (HRDs) are small, bright spots scattered throughout the retina.
- Subretinal Hyperreflective Material (SHRM): Appears as a hyperreflective band between the retina and RPE. Its composition varies but may include fluid, fibrin, blood, and neovascular tissue; it can be associated with poorer visual outcomes.
- RPE Tears: These are disruptions in the RPE monolayer, often occurring in areas of PED. RPE tears can lead to significant vision loss and are an important complication of nAMD.
- Choroidal Changes: nAMD can also affect the choroid, the vascular layer beneath the RPE.
Dry AMD
In its early stages, Dry AMD is characterized by drusen and pigmentary abnormalities resulting from alterations in the retinal pigment epithelium (RPE). Later, it can progress to geographic atrophy (GA) or outer retinal atrophy.
The three classic findings in Dry AMD are drusen, pigmentary changes, and geographic atrophy.
Drusen are classified as:
- small (<65 um),
- medium (65 – 124 um),
- or large (>125 um).
While both drusen and pigmentary changes can appear as yellowish deposits in the retina, pigmentary changes are often more varied in color (ranging from yellow to brown or black) and less defined in shape than the generally circular drusen.
Geographic atrophy typically begins in the paracentral macula, often surrounding the fovea in a horseshoe pattern. It can eventually involve the fovea itself, leading to severe vision loss.
Diabetic Retinopaty (DR)
Diabetic retinopathy (DR), a leading cause of vision loss in working-age populations, is characterized by retinal vascular abnormalities. It progresses from non-proliferative DR (NPDR), marked by vascular leakage and capillary occlusion, to proliferative DR (PDR), where neovascularization can lead to severe vision impairment through vitreous hemorrhage or retinal detachment.
OCT can aid in identifying the earliest sign of DR: microaneurysms. They appear as small, distinct, oval-shaped, hyperreflective, walled structures associated with microvascular damage. Specifically, the structural weakness of the vessel wall of MAs causes fluid leakage, resulting in edema.
Another consequence of microaneurysm formation is the progression to intraretinal hemorrhages (IRH), often called ‘dot-blot’ hemorrhages. These appear as hyperreflective foci on OCT cross-sections, with varying degrees of opacification.
Diabetic macular edema (DME) can occur at any stage of the disease and is the most common cause of vision loss in those with diabetes. It results from a blood-retinal barrier breakdown, leading to fluid leakage and retinal thickening.
Retinal vein occlusions
Retinal vein occlusions (RVOs) are blockages of the retinal veins responsible for draining blood from the retina. These blockages can affect either the central retinal vein (CRVO) or one of its branches (BRVO). RVOs are more prevalent in older individuals and those with underlying vascular conditions such as high blood pressure, high cholesterol, a history of heart attack or stroke, diabetes, or glaucoma. The primary vision-threatening complications of RVO are macular edema, which involves fluid accumulation in the central retina, and retinal ischemia, which results from insufficient blood flow to the retina.
While both Central Retinal Vein Occlusion (CRVO) and Branch Retinal Vein Occlusion (BRVO) involve blockage of a retinal vein, the underlying cause and location of the blockage differ.
CRVO occurs when a thrombus (blood clot) blocks the central retinal vein near the lamina cribrosa, where the optic nerve exits the eye.
In contrast, BRVO typically occurs at an arteriovenous crossing point, where a retinal artery and vein intersect. Atherosclerosis (hardening of the arteries) can compress the vein at this crossing point, leading to thrombus formation and occlusion.
In CRVO, the retina often exhibits extensive intraretinal hemorrhages, dilated and tortuous veins, and cotton-wool spots. This constellation of findings is classically described as a “blood and thunder” appearance. In BRVO, the signs are typically localized to the area of the retina drained by the affected vein. Macular edema, characterized by retinal thickening and cystoid spaces within the retina, is a common finding in CRVO and BRVO and can significantly contribute to vision loss.
Central serous retinopathy
Central serous chorioretinopathy (CSCR) is a common retinal disorder that causes visual impairment and altered visual function. It is classified as a pachychoroid disease, including conditions like polypoidal choroidal vasculopathy and pachychoroid neovasculopathy.
OCT imaging in CSCR often reveals a thicker-than-average choroid.
This diagnostic is particularly useful in cases where clinical examination findings are inconclusive, distinguishing subtle differences between normal and abnormal OCT scans in terms of structural changes, such as small pigment epithelial detachments (PEDs) and hyperreflective subretinal fluid, that may not readily appear on clinical exams.
Furthermore, OCT is valuable for monitoring disease progression and resolution in chronic CSCR cases. A distinguishing feature that can also be seen in CSR is the appearance of the retinal pigment epithelium: the RPE line typically appears straight in non-affected areas, while it can appear wavy or irregular in areas with CSCR.
Epiretinal membrane (Epiretinal fibrosis)
Epiretinal fibrosis (epiretinal membrane/macular pucker) is a common condition affecting the central retina, specifically the macula. It is characterized by a semi-translucent, avascular membrane that forms on the retinal surface, overlying the internal limiting membrane (ILM), which is absent on a normal macula OCT.
OCT plays a crucial role in assessing the severity of ERMs, revealing the extent of macular distortion and the involvement of retinal layers.
OCT findings in ERMs are used to stage the severity of the membrane, ranging:
- Stage 1: ERMs are mild and thin. Foveal depression is present.
- Stage 2: ERMs with widening the outer nuclear layer and losing the foveal depression.
- Stage 3: ERMs with continuous ectopic inner foveal layers crossing the entire foveal area.
- Stage 4: ERMs are thick with continuous ectopic inner foveal and disrupted retinal layers.
Retinal detachment
Retinal detachment is an important cause of decreased visual acuity and blindness, a common ocular emergency often requiring urgent treatment.
It occurs when subretinal fluid accumulates between the neurosensory retina and the retinal pigment epithelium through three mechanisms:
- Rhegmatogenous: a break in the retina allowing liquified vitreous to enter the subretinal space directly.
- Tractional: proliferative membranes on the surface of the retina or vitreous pull on the neurosensory retina, causing a physical separation between the neurosensory retina and retinal pigment epithelium
- Exudative: accumulation of subretinal fluid due to inflammatory mediators or exudation of fluid from a mass lesion/insufficient RPE function
OCT helps identify foveal status and diagnose tractional or exudative retinal detachments, aiding in treatment planning.
Macular hole
Macular holes are full-thickness defects of retinal tissue involving the anatomic fovea and primarily the foveola of the eye. They are thought to form due to anterior-posterior forces, tangential forces and weakening in the retinal architecture that result in openings in the macular center.
The International Vitreomacular Traction Study (IVTS) Group formed a classification scheme of vitreomacular traction and macular holes based on OCT findings:
- Vitreomacular adhesion (VMA): No distortion of the foveal contour; size of attachment area between hyaloid and retina defined as focal if </= 1500 microns and broad if >1500 microns
- Vitreomacular traction (VMT): Distortion of foveal contour present or intraretinal structural changes in the absence of a full-thickness macular hole; size of attachment area between hyaloid and retina defined as focal if </= 1500 microns and broad if >1500 microns.
- Full-thickness macular hole (FTMH): Full-thickness defect from the internal limiting membrane to the retinal pigment epithelium. Described 3 factors: 1) Size – horizontal diameter at narrowest point: small (≤ 250 μm), medium (250-400 μm), large (> 400 μm); 2) Cause – primary or secondary; 3) Presence of absence of VMT.
Glaucoma
Glaucoma is a progressive optic neuropathy that is multifactorial and degenerative. It is characterized by the death of retinal ganglion cells (RGCs) and their axons, leading to the characteristic optic disc and retinal nerve fiber layer (RNFL) structural changes and associated vision loss. One of the most effective ways to get information about nerve states is OCT.
The Glaucoma OCT test provides valuable information about ganglion cells: damage to the ganglion cells or their processes leads to thinning across respective layers, which we can measure as the thickness of the ganglion cell complex.
Key things to focus on when working with OCT for glaucoma detection:
- Look for thinning of the pRNFL, particularly in the inferior and superior quadrants, asymmetrical thinning between a patient’s eyes
- Assess the thickness of the ganglion cell-inner plexiform layer, macular RNFL, and the overall ganglion cell complex.
- Monitoring: Seek significant decreases over time in pRNFL thickness (≥5 μm globally, ≥7-8 μm in specific sectors) or in average GCIPL thickness (>4μm).
AI-powered OCT interpretation tools, such as Altris AI, AI for OCT, can further assist clinicians by providing automated calculations of RNFL thinning in the upper and lower hemispheres and the asymmetry levels between them.
Summing up
OCT has revolutionized ophthalmology, bringing a wealth of new details and challenges. The human eye can easily miss subtle abnormalities on complex scans, making accurate interpretation critical. While experience is essential, relying solely on “learning by doing” poses risks.
AI-powered OCT interpretation software bridges this gap, offering a safety net during the learning curve and beyond. AI-powered second opinion on OCT scans enhances diagnostic accuracy, empowers clinicians, and allows them to spend more time for a meaningful connection with patients.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.
-
Optometry Practice Growth: Business Cases
Altris Inc.
03.10.20248 min readOptometry practice growth: business cases
The client. Dr. William C. Fruchtman’s Optometry Practice, owned and operated by Dr. William C. Fruchtman, O.D., is located in East Rutherford, New Jersey, an inner-ring suburb of New York City. With over 30 years of service to the community, the practice provides comprehensive eye care, including regular eye examinations, contact lenses, and glasses prescriptions.
Dr. William Fruchtman’s practice continually seeks opportunities to add value to its services. He is cultivating his expertise in dry eye disease and macular degeneration, implementing advanced technologies, and using another effective strategy to expand his patient base – communicating with patients in their preferred language. Knowing that clear communication is vital to good care, Dr. William C. Fruchtman’s team includes members who speak Spanish and Polish. As such, their website is available in both Polish and Spanish, a valuable asset considering the area’s substantial Spanish-speaking population (up to 20% of the local demographic).
While achieving fluency in every language spoken within your community may not be feasible, consider adapting your website and patient materials to include translations in commonly spoken languages. As Dr. Fruchtman’s experience confirms, even a simple greeting in a patient’s native language can create a bond with patients or, at the very least, prompt a genuine surprised smile.
The problem. To establish expertise in specialized services, Dr. William Fruchtman has been committed to effectively managing dry eye disease and macular degeneration. Not so long ago, the practice implemented Equinox Low-Level Light Therapy (LLLT). This advanced dry eye treatment utilizes LED lights to warm the eyelids gently, promoting meibomian gland function and oil release. With dry eye management addressed, Dr. Fruchtman sought an additional tool to both strengthen his decision-making when managing patients with other pathologies, particularly macular degeneration, and increase his optometry practice growth.
The solution. After researching Altris AI, an Artificial Intelligence platform for OCT scan analysis, Dr. Fruchtman was positive that he wanted to try the platform. Following introductory meetings and a quick onboarding with the Altris team, he started a two-week trial. After personally testing the platform, Dr. Fruchtman decided it was an invaluable addition to his practice.
Integrating Altris AI into the practice has notably enhanced Dr. Fruchtman’s confidence and precision in diagnosing and managing eye care disorders. The practice has also gained a significant competitive advantage, as the platform can routinely perform Glaucoma Risk Analysis on existing OCT scans, offering additional value to patients.
Thanks to the color-coded and labeled OCTs, optometry facilitates patient education and enables practitioners and patients to monitor the progression or treatment results more effectively.
How to grow an optometry practice: more cases from optometry owners
Optometrists undergo years of education, training, practice, and continuous learning – understandably, it is hard to see additional time or resources to pursue business education.
Many practitioners experience stress, balancing patient care demands with the realities of running a profitable business. This feeling can intensify when attending countless conferences and webinars highlighting thousands of ways to make business more efficient. While they offer valuable advice, it’s sometimes helpful to remember simple points of how successful optometry practice growth will look: attracting new patients, retaining existing ones, and ensuring a smooth and efficient workflow. These (even though overly simplified) points allow you to focus on the most critical details.
But before diving into ways of optometry practice growth, remember that the first step is a realistic assessment of your current situation.
While you’re likely aware of some issues, feedback from your team and patients can provide insights, and sometimes even immediate solutions, for areas of improvement.
Even though we cannot directly assist in assessing your specific practice, as you know it best, below we offer some key, proven strategies for growing your business.
Optometry practice growth: expanding your patient base
- Dry Eye Specialization
One effective strategy for optometry practice growth is to expand the scope of services to include the diagnosis and management of ocular diseases. For example, dry eye disease (DED) affects ∼344 million people worldwide and over 20 million in the United States alone, yet many remain undiagnosed and untreated. This presents a significant opportunity to care for a large and often underserved patient population. By developing expertise in DED and offering specialized treatments, you can not only attract new patients but also contribute to improving the quality of life for those suffering from this chronic condition.
There are numerous approaches to managing DED effectively. As mentioned, Dr. William C. Fruchtman’s practice utilizes Equinox Low-Level Light Therapy (LLLT).
Dr. Shane Swatts, O.D., owner of Eastern Virginia Eye Associates, employs AI software to enhance DED diagnostics, conduct more comprehensive analyses, and keep detailed patient medical histories. This technology upgrades pre-and post-operative care, saving time without compromising accuracy.
- Aesthetic Optometry
Dr. Janelle Davison identified an opportunity for optometry practice growth by addressing patient needs while generating additional revenue by incorporating aesthetic optometry services into her practice. Within a single quarter, her practice generated $14,000 in revenue from aesthetic product sales alone.
Dr. Davison also collaborates with a licensed aesthetician who operates within the practice on a contract basis, sharing the revenue generated from aesthetic services.
- Glaucoma Management
Dr. James Deom, O.D., M.P.H., an optometrist from Pennsylvania, implemented a successful strategy for optometry practice growth based on attracting glaucoma patients, significantly increasing glaucoma-related revenue. He initiated internal marketing efforts by inquiring about patients’ family history of glaucoma and informing them about the practice’s newest technology for the early detection of vision loss.
Practices specializing in glaucoma management can significantly benefit from incorporating advanced software solutions to complement their existing diagnostic hardware. For instance, integrating Altris AI, AI for OCT, into their OCT analysis workflow enables not only automated screening of 70+ pathologies and biomarkers but includes assessing retinal nerve fiber layer (RNFL) asymmetry for glaucoma risk evaluation.
- Patient-Centered Care
Offering diverse channels for patient interaction can broaden your practice’s reach and improve the patient experience. Dr. Melissa Richard, O.D., sought to provide patients with a preview of frame options before their appointments. To achieve this, she integrated Optify technology into her practice, a solution she discovered during a Vision Source Exchange lecture. This technology creates a virtual showroom where patients can explore and select their preferred frames in advance, streamlining the in-office experience.
Patient education is also key to patient-centered care and personalization, which not only empowers individuals and improves their outcomes but also fosters optometry practice growth. Those who understand their eye health are more likely to adhere to recommendations.
A study demonstrates that 94% desire educational content, but a third don’t receive it.
Providing color-coded OCT reports with pathologies, biomarkers, and pathology progression tracking not only satisfies this need but also elevates your practice above competitors.
Improve efficiency in the optometry office through strategic partnerships & team building
When optometrists consider further career development, they may seek additional support to achieve their goals. Dr. Linda Enciso, O.D., found such support when her practice joined the AEG Vision family in 2019. The transition brought numerous positive changes, boosting patient care and fostering growth opportunities for team members.
Although Dr. Enciso had already been operating her practice for 13 years and had implemented electronic health records (EHR) systems and third-party software to improve patient communication and boost optometry practice growth, her goal was to continue these advancements and expand the scope of practice. Joining AEG Vision allowed her to transition to the training team, access continuing education opportunities to stay informed about advancements in optometry and healthcare, collaborate with other healthcare providers and cross-functional teams to enhance comprehensive patient care.
While the phrase “team building” might evoke images of complicated activities and extensive effort, fostering a strong team can be achieved through simple, engaging initiatives. Consider the inspiring example of Dr. Jonathan Cargo, O.D.
Dr. Cargo recognizes the value of personal development through reading but finds it challenging to share his insights with his team effectively. Inspired by his wife’s long-standing book club, he initiated an office book club to encourage team connection and shared learning to improve efficiency in the optometry office.
The book club operates with team members suggesting relevant titles and collectively reading chapters over a month, dedicating time during team meetings for discussions. Dr. Cargo highlights the recent success of reading “Crucial Conversations,” a selection prompted by team members’ desire to deepen their communication skills, particularly in navigating challenging discussions with colleagues, patients, and even family members. The shared reading experience gave a better understanding of effective communication strategies and empowered the team to navigate difficult conversations.
Summing up
When regarding optometry practice growth, consider the time, effort, and resources you are prepared to invest. To expand your patient base, explore the addition of new services.
To optimize costs and efficiency and gain a competitive edge, investigate the possibility of implementing AI in your practice – it can be a second-opinion tool, or you can read here how practitioners use it for marketing, creating educational materials, and more. To encourage staff retention and nurture a positive work environment, prioritize team-building activities; even seemingly simple initiatives can produce significant benefits.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.
-
Optometry Trends in Action: 12 Real-World Success Stories
Maria Znamenska
17.09.20248 min readOptometry Trends in Action: 12 Real-World Success Stories
Optometry trends explained: showcasing real-world optometry practice owners who are adapting to the shift in patient needs, successfully implementing solutions to automate routine and laborious tasks, using AI to combat staff shortages, creating their own brand mascots, and more.
Optometry trends for the patient journey: digital communication
Online shopping, global deliveries, and instant brand replies through messengers have dramatically shifted client expectations and behaviors. The ‘convenience economy’ isn’t slowing down, pushing businesses to adopt technology for more streamlined consumer experiences.
What does this mean for your practice? Your patients now expect fast and efficient communication across all touchpoints – from online scheduling to contactless payments. Transforming your practice to meet these demands ensures satisfied patients and contributes to long-term success, as any optometry practice thrives on the individual experiences of the patients it provides.
46% of optometrists reported that patient expectations have risen since the pandemic.
Practices can optimize their workflows in various ways, but generally, the goal is to automate routine administrative tasks, free up staff, and reduce patient waiting time. Digital safety forms and document management systems eliminate physical paperwork, while online proofing and approval systems speed up document processing.
Dr. Justin Bazan, owner and optometrist at Park Slope Eye, New York, has taken this even further by eliminating phone calls at his office entirely and is pleased with the results. This solution was based on several months of analyzing data related to phone calls, including time spent on calls and the frequency of missed calls. The team recognized that while the staff could simultaneously chat with multiple patients, they could only handle one phone call at a time.

Chad Fleming, OD, Owner and OD at Wichita Optometry, Kansas, also identified the need for an enhanced digital presence to prioritize patient convenience. His practice faced the challenge of managing a high volume of phone calls and text messages, requiring either additional staff hiring without an immediate increase in revenue or a strategic reallocation of existing personnel.
Dr. Fleming optimized the patient experience by setting up automated checkouts at some of his practice locations. This approach enabled him to reassign three front desk employees to the digital communications team. While the transition required patient education to familiarize them with the virtual check-in process on iPads, it did not result in patient attrition.
Brianna Rhue, OD, Owner and Optometrist of West Broward Eyecare Associates, Florida, agrees that the traditional approach of answering calls and checking emails once a day differs from today’s patient expectations. She advocates step-by-step optimizations throughout the patient journey to eliminate unnecessary wait times and increase productivity.
Upgrading to a more advanced EHR system is one of the significant opportunities to streamline practice operations, save practitioners time, money, and stress, and align with optometry industry trends. Unfortunately, once hailed as revolutionary, some widely adopted EHR solutions are now criticized for their burdensome workflows and counterintuitive interfaces. This has led some practitioners to describe their interaction with systems as “death by a thousand clicks.”
By leveraging up-to-date EHR features like customizable patient encounter templates, integrated imaging and diagnostic tools, and patient outcome tracking, eye care professionals can shift their focus from paperwork to patient care.
Another of optometry trends gaining momentum among optometry practice owners is offering flexible payment options. This reflects not only the growing demand for convenience but also the financial constraints of patients navigating the current economy that is heading to a recession.
Dr. Rhue encourages practices to adopt mobile payment solutions that enable patients to pay electronically using platforms like Apple Pay, Venmo, or PayPal at the point of service. For balances due after the visit, the ability to send secure payment links via text message can greatly enhance the collection process.
Furthermore, providing patient financing options empowers patients to choose how and when they pay. This offers additional convenience for both parties and eliminates friction by allowing patients to spread the cost of their care over time rather than requiring full payment upfront.
If you are still determining which technologies of these optometry industry trends your patients will be eager to adopt, consider the approach taken by Scott Jens, OD, the owner of Isthmus Eye Care, Wisconsin. Dr. Jens has successfully implemented post-examination surveys to gather patient feedback. This strategy serves a dual purpose: demonstrating your commitment to patient satisfaction and gaining valuable insights into which technological advancements would most benefit your practice.
Optometry trends in the exam room: tech-driven precision and patient education
Optometry relies heavily on technology, and investing in hardware upgrades is a significant financial commitment. However, if your hardware needs are met, but you still want to be at the forefront of technological advancements, consider specialized software and platforms to extend the possibilities of your existing devices.
Dr. Maria Sampalis, OD, the owner of Sampalis Eye Care, Rhode Island, utilizes two such programs in her practice. To support her specialization in dry eye management, she employs CSI Dry Eye. Additionally, she uses Altris AI, an AI-powered platform for OCT scan analysis, to provide a second opinion and enhance diagnostic accuracy.
Dr. Sampalis finds that the Dry Eye software allows her and her staff to analyze symptoms and images comprehensively, improving patient care, time savings, and increasing diagnostic precision. See how OCT AI works here.
Her patients also appreciate Altris AI, which analyzes OCT scans for over 70 pathologies and biomarkers while also calculating the risk of developing glaucoma.
Working with specialized software solutions improves diagnostic accuracy and aids in patient education. Visual representations of their conditions, facilitated by these technologies, empower patients with a clearer understanding, leading to increased treatment compliance.

Eye Place, an optometry center in Columbia, also leverages Altris AI, among other cutting-edge technologies. They capture images using the Topcon Maestro2 OCT and use Image Net6 software to export DICOM files to the Altris AI platform.
Beyond AI-powered OCT analysis, Eye Place utilizes state-of-the-art diagnostic tools, such as 3D OCT equipment, to screen for serious conditions, including glaucoma, diabetes, and macular degeneration. Furthermore, they work with AdaptDX Pro, a technology capable of detecting macular degeneration earlier than traditional methods.
Another case of optimizing and enhancing the exam process is West Broward Eyecare Associates. They implemented Optify, a smart building solution offering full fiber connectivity. Patients can pre-select frames in the online optical store before their visit, streamlining the in-office experience. Additionally, the practice utilizes Dr. Contact Lens, a platform for convenient ordering, reordering, and prescription management for contact lens wearers, reducing paper waste.
There are also advancements in AI transcription technology that are poised to ease clinical documentation and automate a traditionally laborious task.
The adoption of AI in clinical documentation has been shown to reduce the time doctors spend on charting by approximately 2 hours per day.
AI exam transcription is still in the process, and the existing possibilities are not yet flawless—struggling with patient responses like “mm-hm” and “uh-huh”—the technology is evolving, promising greater efficiency and accuracy in the future. For example, one such program starts the transcription process of the exam by confirming patient consent and a click of the record button by the optometrist. Then, AI captures, structures, and summarizes information in real-time, filtering for relevant details to generate documentation for each patient appointment.
Optometry trends for competitive advantage: using AI in Marketing and Decision-making
Some practice owners may still believe their patient demographics do not necessitate an expanded online presence, particularly when considering elders. But you should be different from your competitors.
The reality is that today’s patients, regardless of age, are increasingly turning to the Internet for information and services. While word-of-mouth referrals remain valuable, a solid online presence is essential for practice growth and visibility in today’s competitive landscape.
Twin Forks Optometry and Vision Therapy in New York reports that their most effective marketing strategy involves a monthly-to-quarterly newsletter distributed to existing patients. This newsletter highlights practice updates, recent vision therapy graduates, new podcast episodes, and seasonal information. They’ve also observed that educational posts generate significant engagement and have even led to new patient visits.
Voice Search Optimization (VSO) is emerging as one of the new trends in optometry that has the potential to benefit practices significantly. Dr. Brianna Rhue, OD, co-owner of West Broward Eyecare Associates in Florida, asserts that a search engine optimized (SEO) website alone will soon be insufficient for patients to discover your practice online easily, especially in highly competitive locations.
Contrary to popular belief, it’s not just the tech-savvy individuals who rely on voice assistants. This technology is predominantly used by older individuals who haven’t mastered typing or face difficulties with it.
However, while the benefits of digital communication are undeniable, it’s crucial to acknowledge that it often adds up yet another layer of responsibility to already overburdened teams. This is why generative AI tools like ChatGPT and Gemini are gaining popularity among optometrists, offering solutions to this and other challenges.
For example, Dr. Ryan Cazares, the owner and founder of Scott Eye Care in Louisiana, utilizes ChatGPT to generate social media and educational content for his practice. He brainstorms with AI content ideas, creates visuals for social media and marketing campaigns, and has even developed a unique mascot (Dr. Seymour) that engages his audience.
The practitioner also uses AI to generate personalized educational materials for their patients. Traditionally, his practice relied on generic Optometric Association pamphlets, but now, it has transitioned to simple one-page educational sheets tailored to individual patient needs.
Dr. Haley Perry, owner of Elite Eye Care, New York, provides another example of AI’s potential in practice management. Her goal for this year was to increase patient volume without expanding her staff, and ChatGPT played a pivotal role in achieving this objective.
Faced with the decision between two vendors for new exam room equipment, she used AI to analyze each vendor’s pricing and financing options, weigh the pros and cons of the equipment in relation to her goals, and forecast the return on investment (ROI) for each option. This analysis enabled her to select the most suitable vendor and estimate the timeframe for recouping her investment.
Dr. Perry also leverages AI to analyze patient feedback, demographic data, and treatment outcome statistics to ensure equipment investments align with patient needs. For instance, if data reveals a high prevalence of conditions like glaucoma, AI can help justify investing in advanced glaucoma screening tools.
Summing up
The optometry landscape is evolving, driven by raised patient expectations for convenience and efficiency. Practices adapt to these changes by embracing emerging optometry trends to achieve more precise diagnostics, streamline patient journeys, enhance the exam room experience, and build trust and connection. Much of this technology is AI-based, with even more advancements on the horizon. So, optometrists implementing these solutions today are poised to secure a significant competitive advantage.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.
-

Optometry Technology: What to Expect?
Maria Znamenska
7 min.7 min.Optometry Technology: What to Expect?
For this article, we surveyed eye care professionals on which optometry technology appears most promising to them. The answers were divided among AI for more precise diagnostics, advanced contact lenses, and new iterations of OCTs.
Of course, this is not the whole list of possible new tech in optometry, but these are the topics that draw the most attention today.
The article delves deeper into each of these technologies, as well as explores oculomics, the new way of understanding the correlation between eye pathology and overall human health.
New tech in optometry: AI for Medical Image Analysis
AI has blossomed in recent years, transforming not only how we work and relax but also how we manage our health. It’s no surprise that our survey of professionals revealed AI as the most promising technology in optometry.
The most immediate and practical AI implementation in optometry is the analysis of medical images, such as fundus photos and OCT scans.
They require no additional equipment beyond the OCT and fundus cameras many practitioners already own, are cost-effective, and add huge value to a practice.
There are many companies that detect a number of biomarkers and help with diagnostic decision-making already, and their number will only increase from year to year for several reasons:
- AI systems for medical image analysis speed up patient triage
- AI systems help to detect early, minor, and rare pathologies which sometimes can be missed
- AI systems help with complex cases when a second opinion is needed
- Quantitative analysis of biomarkers improves treatment results monitoring making it more efficient
For instance, AI today can assess the early risk of glaucoma based on the GCC asymmetry measurements. Here is how AI-powered OCT workflow would look.
AI-assisted readings of OCT scans are already helping not only with pathology detection but also with the analysis of its progression or response to treatment. This represents a new approach to monitoring, where practitioners no longer need to sift through various patient notes but can directly compare reports from previous examinations and observe how, for instance, shadowing has changed in micrometers.

AI programs are becoming even more invaluable with an aging population, as diseases prevalent in older individuals become increasingly common while ophthalmology and optometry face a shortage of specialists. This situation will transform the optometrist’s role, with AI empowering practitioners with the diagnostic capabilities to manage many conditions without referral. This will benefit patients, enabling timely routine screenings and diagnoses and preventing months-long waits that can sometimes lead to irreversible blindness.
AI systems are also being implemented in ophthalmic trials for biomarker detection, exploring the relationship between imaging biomarkers and underlying disease pathways. For instance, a recent study linked levels of various cytokines, including VEGF, MCP-1, and IL-6, with specific OCT-derived biomarkers like fluid parameters and outer retinal integrity.
This significantly accelerates the research process, assisting in identifying the right target audience based on OCT scans, eliminating manual data annotation, and revealing the subtlest changes, progression or regression, and patient responses during trials.
While material advancements allow us to build more precise machines, the new tech in optometry likely won’t involve some unheard-of device. Instead, AI software will enable us to extract the maximum potential from the technologies we already use.
New Tech in Optometry: New Iterations of OCT
Even though OCTs entered the market relatively recently, they swiftly became indispensable ancillary tests in ophthalmic practice for many professionals. The primary reason is their high-quality imaging of the retina, nerve fiber layer, and optic nerve, offering a near in-vivo “optical biopsy” of the retina.
However, the technology continues to evolve – partly due to technological advancements and partly due to the ability to extract even more data from OCT machines through sophisticated software.
SD-OCT is undergoing continuous development, expanding its range of applications. Multimodal imaging, which combines SD-OCT with other imaging techniques like autofluorescence and angiography, now allows for improved diagnosis and management of a wider array of diseases.
Several prominent OCT evolutions combine technological advancements and promise widespread adoption. They are:
New Tech in Optometry: En-face OCT
En-face OCT in current systems is based on software reconstruction of OCT images. Image slices are selected retrospectively from full recorded volumes or calculated by depth projection along specific depth ranges, enabling three-dimensional data visualization in a fundus projection. This technique allows the projection of specific retinal and/or choroidal layers at a given depth onto an en-face view.
While we are more accustomed to working with cross-sectional images (B-scans), microstructural changes and the retinal and choroidal vasculature morphology are challenging to evaluate using B-scans alone. En-face OCT offers numerous advantages, including the ability to precisely localize lesions within specific subretinal layers using their axial location on OCT cross-sections and to register projected OCT images to other fundus imaging modalities using retinal vessels as landmarks.
Currently, en-face OCT is being applied to various specialized areas within the eye, encompassing the anterior segment, glaucoma, infectious diseases, and the retina.
Optometry Technology: SS-OCT
Like SD-OCT, swept-source OCT (SS-OCT) utilizes Fourier domain technology to optimize higher-quality wavelength transduction within the frequency domain. This enables rapid sweeping scan patterns across a broad bandwidth.
However, instead of a broad-bandwidth light source projected all at once, as in SD-OCT, SS-OCT employs a single tunable laser that sweeps through different frequencies to cover the entire spectrum swiftly. The light reflected from the eye is captured by a photodetector significantly faster than the charge-coupled device (CCD) camera used in SD-OCTs. This difference translates to a faster scanning speed of up to 400,000 axial scans per second, eliminating the typical depth-dependent signal drop-off associated with SD-OCT. Additionally, the faster scanning speed reduces image distortions caused by eye movements and allows for wider B-scans, facilitating widefield imaging.
Furthermore, many SS-OCT systems utilize a light source centered at an approximately 1050 nm wavelength, providing better tissue penetration than SD-OCT. This allows for visualization of structures like the choroid, lamina cribrosa, and structures at the anterior chamber angle. This enhanced penetration is crucial in diseases like Central Serous Chorioretinopathy, where evaluating the entire thickness of the choroid can be challenging.
Moreover, volumetric analysis of the choroid and various pathological features can aid in monitoring the progression of Wet AMD, CSCR, and Diabetic Retinopathy, as well as assessing the response to treatments such as anti-VEGF agents, laser photocoagulation, and photodynamic therapy (PDT).
Optometry Trends: OCT Angiography
Given that many ocular diseases are associated with vascular abnormalities, the ability to visualize and quantify blood flow in the eye is crucial. Traditionally, fluorescein angiography (FA) and indocyanine green angiography (ICGA) have been used for this purpose, but these procedures require intravenous injection of contrast agents, which is not only time-consuming but may lead to allergic reactions or potentially serious side effects.
OCTA, on the other hand, produces high-resolution, 3D angiograms of the retinal and choroidal vascular networks, taking advantage of the eye’s unique characteristic as the only organ allowing noninvasive, direct observation of its blood vessels’ structure and function. OCTA detects blood flow using intrinsic signals to capture the location of blood vessels. While it has limitations such as insensitivity to leakage and a relatively small field of view, the development of OCTA has the potential to significantly enhance our understanding of the eye’s physiology and pathophysiology, providing depth-resolved angiographic maps of the tissue’s vascular structure down to the capillary level.
OCTA is particularly valuable in clinical settings where pathologies like diabetic retinopathy, age-related macular degeneration, retinal vein occlusions, and macular telangiectasia are frequently encountered. These conditions often alter blood flow or the blood vessels themselves in the retina, making imaging these vessels essential for diagnosis and management.
Wide-Field and Ultrawide-Field OCT (WF-OCT and UWF-OCT)
While OCT is a powerful ocular imaging tool, it has traditionally been limited by a relatively narrow field of view (FOV) – typically around 20 degrees × 20 degrees. To address this limitation, two advancements have emerged:
- Wide-field OCT (WF-OCT) with an FOV of approximately 60-100 degrees captures the retina’s mid-periphery up to the posterior edge of the vortex vein ampulla.
- Ultrawide-field OCT (UWF-OCT) with an FOV of up to 200 degrees, mapping the far periphery of the retina, including the anterior edge of the vortex vein ampulla and beyond.
WF-OCT provides additional information compared to routine 6-9 mm scans in conditions such as diabetic retinopathy (DR), central serous chorioretinopathy (CSCR), polypoidal choroidal vasculopathy (PCV), peripapillary choroidal neovascular membrane (CNVM), or uveitic entities. It facilitates easier visualization of anatomical details of peripheral retinal changes like ischemic areas in DR, retinal vein occlusions, or sites of retinal breaks, peripheral retinal detachment, retinoschisis, and choroidal lesions (melanoma, nevus, hemangioma, choroidal metastasis).
As with other OCT iterations, WF and UWF OCT will likely provide the most significant insights when routinely combined with other modalities, such as OCT angiography.
New Tech in Optometry: Advanced contact lenses
In our lifetime, contact lenses have evolved from mere corrective devices to sophisticated optical instruments. There are several ways that contact lenses (CLs) continue to advance:
- Manufacturing optimization: Automation and robotization of the process for higher precision and a shift towards a more environmentally friendly approach.
- Design: More precise designs tailored to the wearer’s eye with the help of 3D printing.
- Material advancements: Nanotechnology/surface modifications for improved wettability, lubricity, and antimicrobial properties. Increased focus on biomimetic design.
- Technological advancements: Smart lenses with thin and ultra-thin transistors capable of reacting to or registering the wearer’s stress levels, glucose levels, etc.
Let’s take a closer look at a few examples of Smart Contact Lenses (SCLs) that combine some of the characteristics mentioned earlier.
SCLs are wearable ophthalmic devices that offer functions beyond vision correction. These devices are integrated with sensors, wireless communication components, and microprocessors to measure biological markers. They can treat ocular pathologies by delivering drugs, light, heat, and electrical stimulation, or they can aid in diagnosing. Currently, some SCLs can help manage glaucoma, cataracts, dry eye syndrome, eye infections, and inflammation. In development are lenses to treat age-related macular degeneration (AMD), diabetic retinopathy (DR), retinitis, and posterior uveitis. An artificial retina (retinal prosthesis) is in its early developmental stage, with the potential to restore vision to some degree for specific types of blindness caused by degenerative diseases.
Scientists from the School of Medical Sciences in New South Wales have implanted epithelial stem cells (ESCs) from a healthy eye into a contact lens. This innovation has shown promise in repairing vision loss caused by a damaged cornea. In another breakthrough, scientists from Oregon State University have utilized ultra-thin transistor technology to design SCLs that can monitor the wearer’s physiological state. While this futuristic contact lens is still in the prototype phase, several biotech companies have already expressed interest in its development.
Smart lenses also show great promise in drug delivery. One of the main challenges with eye drops is their low bioavailability (less than 5%), primarily due to high tear turnover rates, blinking, nasolacrimal drainage, non-productive absorption by the conjunctiva, and the cornea’s low permeability. Therefore, improving bioavailability by increasing the drug’s residence time on the ocular surface remains a critical research focus.
Additionally, drug delivery via SCLs can offer more precise dosing. With traditional eye drops, dosage accuracy relies on the patient’s ability to tilt their head and squeeze the inverted bottle correctly, leading to inconsistent application. Consequently, compliance rates for eye drops are low. In contrast, the drug delivery process with SCLs involves lenses loaded with medication for a day or several days, potentially enhancing compliance, especially for individuals accustomed to wearing contact lenses as part of their routine.
Just as artificial intelligence is merging with ophthalmic devices for detection and analysis, opening new possibilities, optometry trends are also venturing contact lenses into the multidisciplinary field of theranostics, which combines therapeutics and diagnostics. This field is uncovering new avenues of research, shedding light on disease mechanisms, and driving drug and medical device development. Theranostics leverages knowledge and techniques from nanotechnology, molecular and nuclear medicine, and pharmacogenetics to achieve goals such as in vitro diagnostics and prognostics, in vivo molecular imaging and therapy, and targeted drug delivery. This approach is shifting patient care towards proactive strategies and predictive treatments.
Optometry Technology: Oculomics
For decades, researchers have sought to measure retinal changes to identify ocular biomarkers for systemic diseases, a field now known as oculomics.
As mentioned earlier, the eye provides a unique opportunity for direct, in vivo, and often non-invasive visualization of the neurosensory and microvascular systems:
- The eye shares a common embryological origin with the brain, and the neurosensory retina and optic nerve are considered extensions of the brain, allowing direct observation of the nervous system.
- Due to the length and continuity of the visual pathway, along with trans-synaptic degeneration mechanisms, damage to the central nervous system often manifests as changes in the inner retina.
- The blood-retina barrier, similar to the blood-brain barrier, selectively allows the transport of essential substances to these metabolically active structures.
- The aqueous and vitreous humors are plasma-derived and transport lipid-soluble substances through diffusion and water-soluble substances through ultrafiltration.
- The lens, which grows continuously throughout life, accumulates molecules over time, providing a potential map of an individual’s molecular history.
The link between the eye and overall human health is not new. However, with the increasing availability and complexity of large, multimodal ocular image datasets, artificial intelligence-based ocular image analysis shows great promise as a noninvasive tool for predicting various systemic diseases. This is achieved by evaluating risk factors, retinal features, and biomarkers. Thanks to the massive datasets generated through recent ophthalmic imaging, which are now being used for deep learning and AI training, oculomics is starting to yield more precise answers. For example, the NHS alone has been conducting eye tests for over 60 years, resulting in databases containing millions of images, complete with patient records and long-term health outcomes. These datasets have been fed into AI algorithms, leading to models that can already predict cardiovascular risk factors with accuracy comparable to the current state-of-the-art methods.
It’s a significant opportunity because, with the aging population, a primary healthcare focus will be not only extending lifespan longevity but also maintaining crucial healthspan functions. The primary obstacles to both longevity and healthspan are chronic diseases, referred to as the “Four Horsemen of Chronic Disease” (Cardiovascular disease, Cancer, Neurodegenerative disease, and Metabolic disease). Many of these can be, if not entirely prevented, at least minimized in terms of progression through timely detection and intervention.
One major advantage of discovering biomarkers that can predict diseases is that eye screenings are generally less intimidating than other procedures. For example, a person might regularly visit an optometrist for prescription glasses but avoid routine cervical screenings. A less anxiety-provoking and familiar procedure could significantly impact healthcare engagement. Such screenings could also make a substantial difference for chronic conditions like dementia, diabetes, and cardiovascular disease, which constitute a significant portion of the “burden of disease.”
Summing up
Artificial intelligence has already significantly impacted our lives. It holds immense promise in optometry technology, as its primary capability—analyzing massive datasets—aligns perfectly with eye care, where thousands of images are generated daily. Training on such vast amounts of data will lead to breakthroughs in pathology and biomarker detection and their correlation with overall human health. It will enable us to take a giant leap towards proactive and predictive medicine, helping our patients live longer, healthier lives.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.
-

Altris Announces Appointment of Grant Schmid as a VP of Business Development
Altris Inc.
26.08.20241 min.Altris AI Announces the Appointment of Grant Schmid as the VP Business Development
Altris AI, a leading AI software provider for OCT scan analysis, announces the appointment of Grant Schmid as the Vice President Business Development. Mr. Schmid is a proven leader in the eye care industry and has solid experience that will help him establish new partnerships for the company and lead corporate sales.
The recent surge in AI (artificial intelligence) applications across industries has transformed the technology landscape, especially in healthcare. While AI companies have existed for years, the explosion of tools like ChatGPT has popularized the integration of AI in everyday processes.
Grant was drawn to Altris AI for its focus on harnessing AI capabilities to assist doctors in making faster and more informed decisions.
According to Mr. Schmid,
“Healthcare professionals are inundated with more data than most other professions, particularly in the eye care segment. Eye care specialists are subjected to multiple tests and instruments, generating a vast amount of data that must be reviewed comprehensively. A single Optical Coherence Tomography (OCT) test can contain over five hundred thousand data points. This necessitates that doctors carefully analyze results from various tests, often overlapping with different devices, which can be time-consuming and detract from the time they have with their patients.”
At Altris AI, the mission is not to replace the vital human connection in medicine but to enhance it.

Grant also remarked that,
“Some AI companies are positioning their products as replacements for human doctors, which undermines the essential aspects of patient care. Patients need to feel heard, and doctors choose this profession to help individuals. Altris AI enables doctors to spend more time with their patients, allowing them to focus on the human aspects of care rather than getting lost in data analysis.”
About Altris AI.
Altris AI is a part of the Altris Inc. ecosystem that includes Altris AI( a standalone AI platform for OCT scan analysis that improves diagnostic decision-making for eye care specialists) and Altris Education OCT (a free mobile app for OCT education interpretation). The mission of the company is to set higher diagnostic standards in the eye care industry and improve patient outcomes as a result. To achieve this mission the company created an AI-powered platform for OCT scan analysis that detects the biggest number of biomarkers and retina pathologies on the market today: 70 + including early glaucoma. More than that, the company offers an automated quantitative analysis of biomarkers and a progression analysis module for monitoring treatment results more efficiently.
Disclaimer: USA FDA 510(k) Class II; Altris Image Management System (Altris IMS); AI/ML models and components intended to use for research purposes only, not for clinical diagnosis purposes.

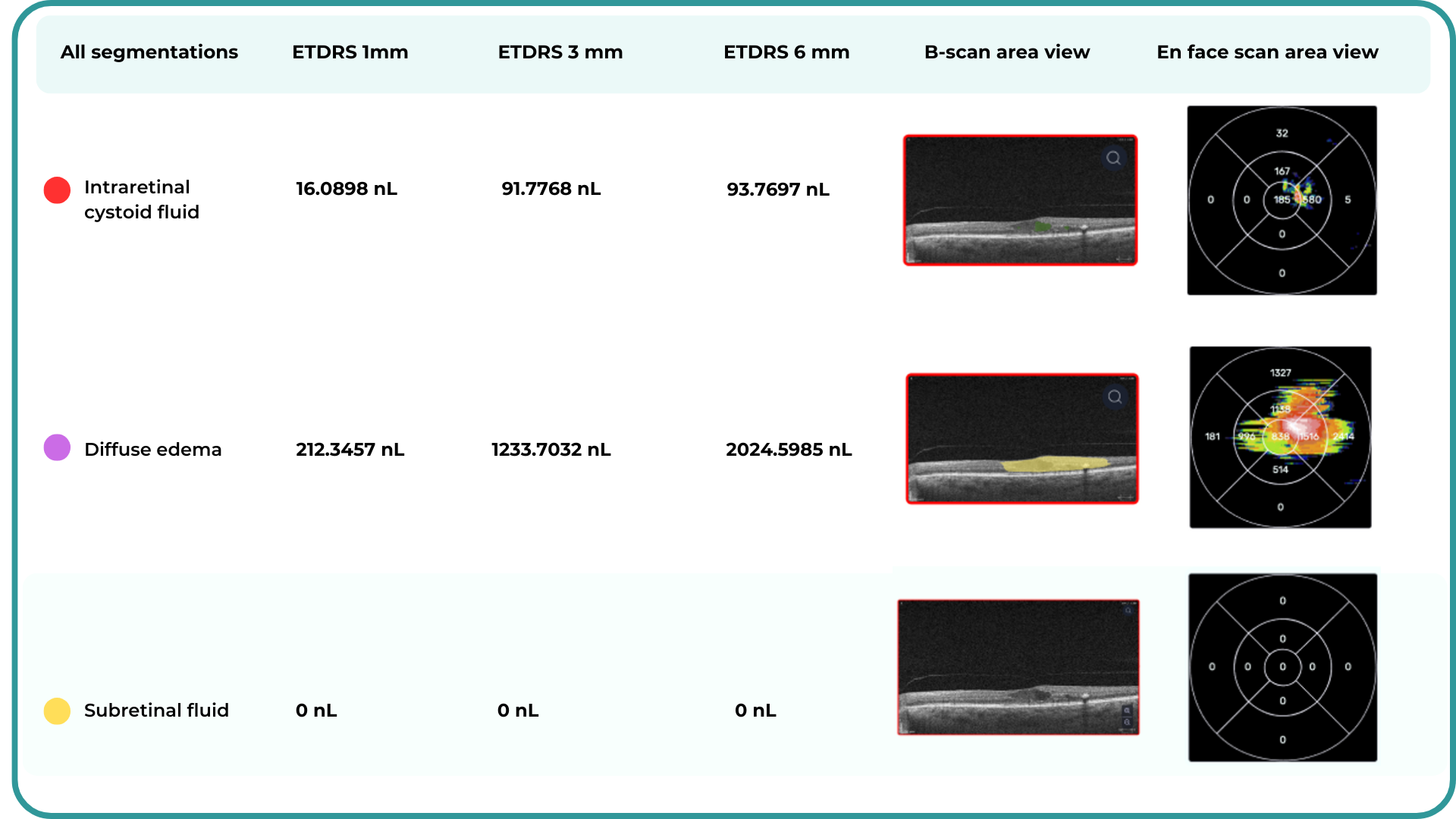
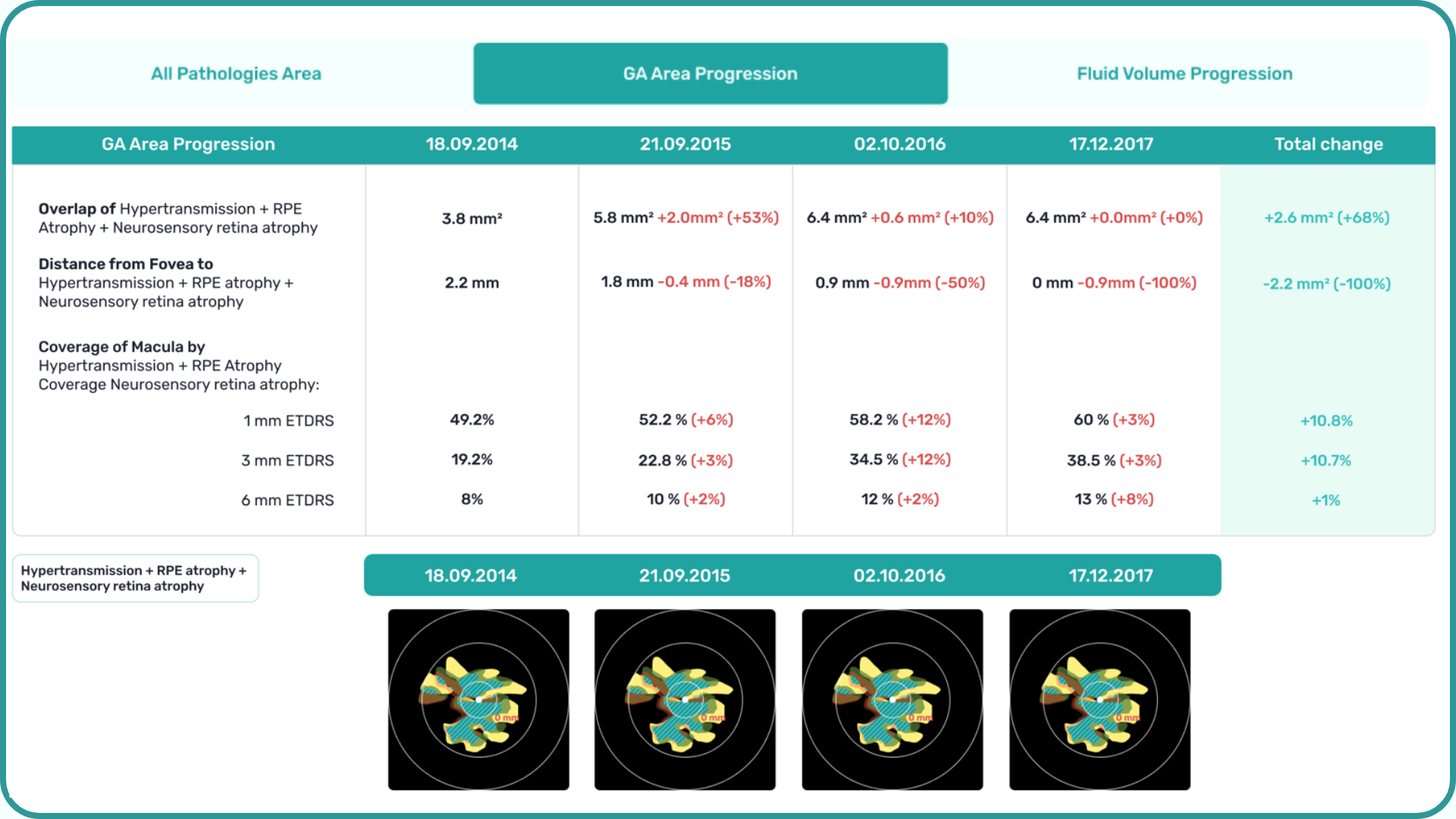
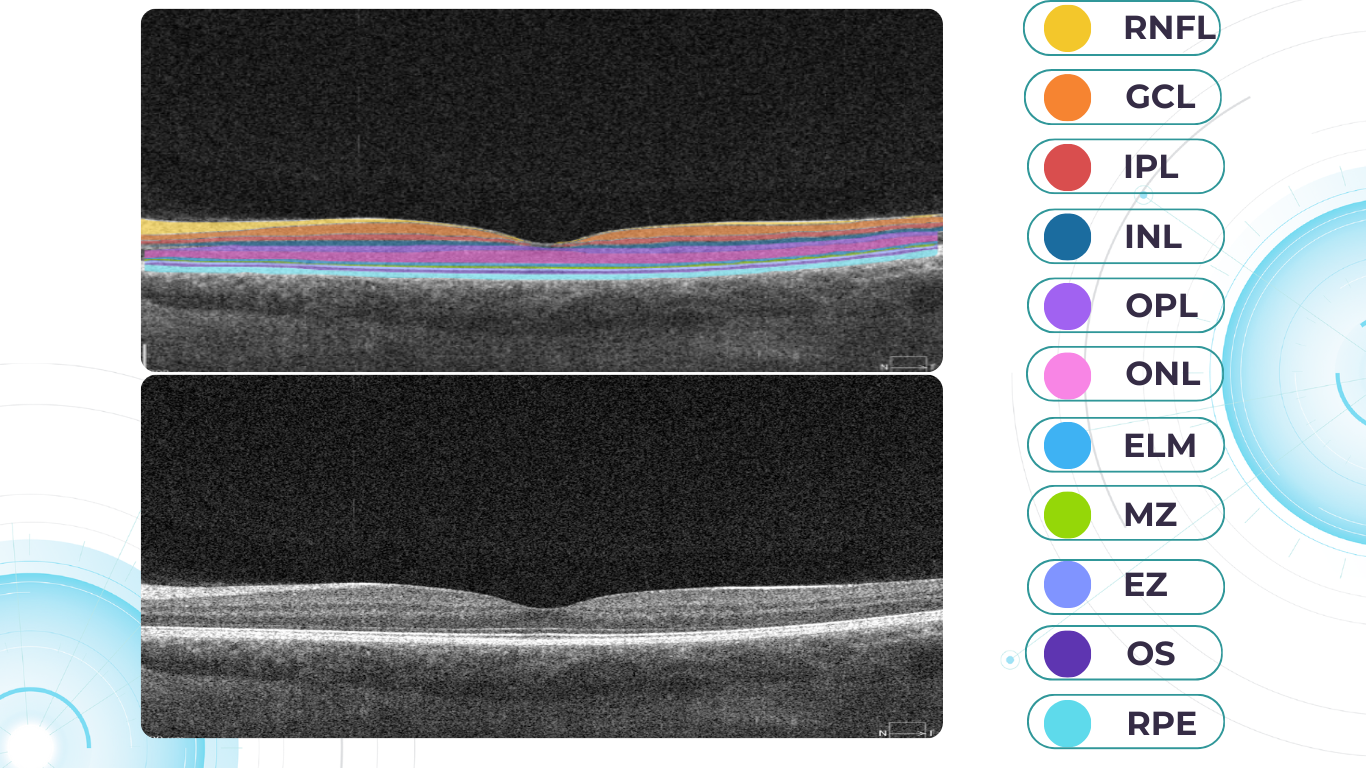
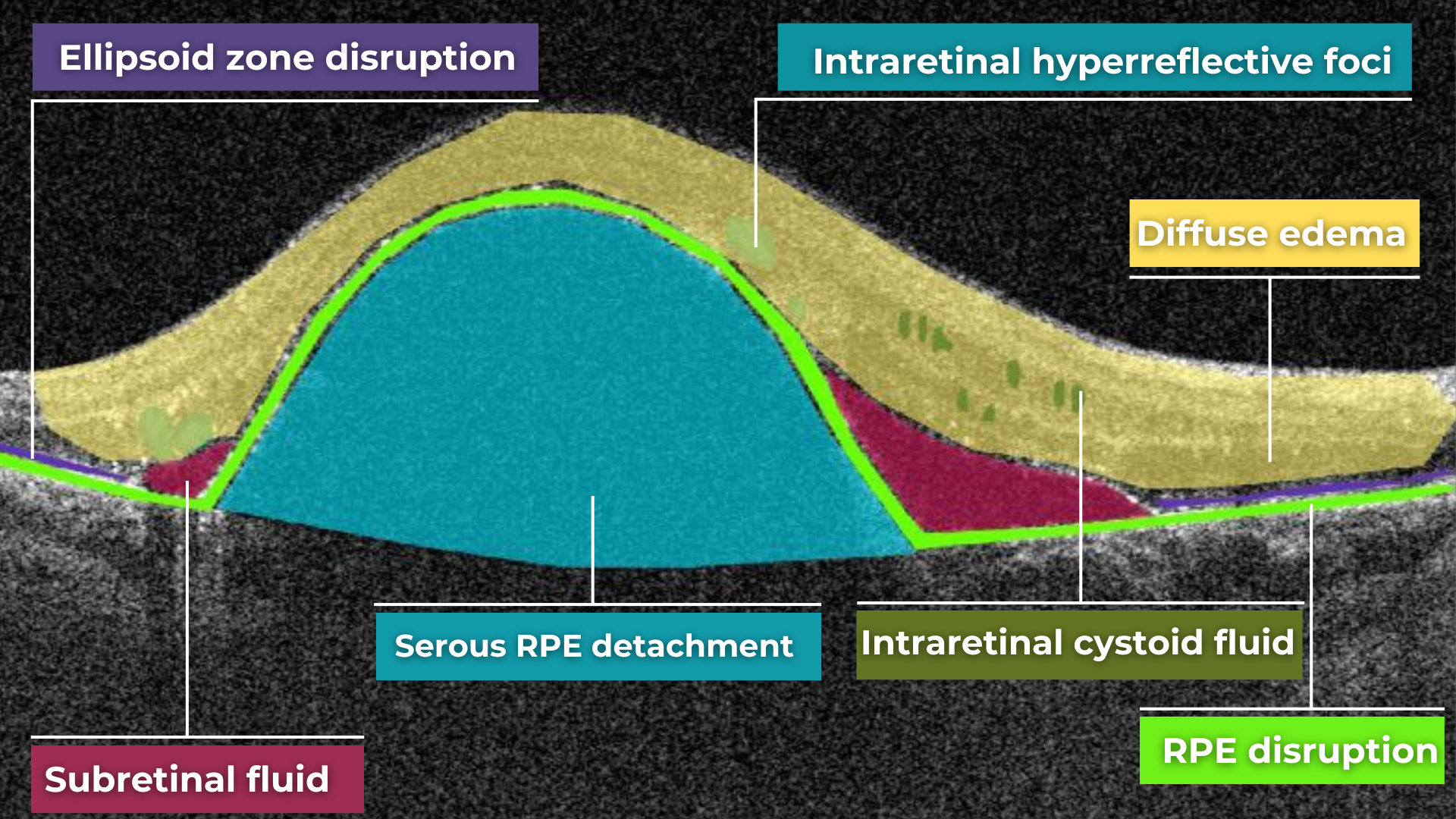
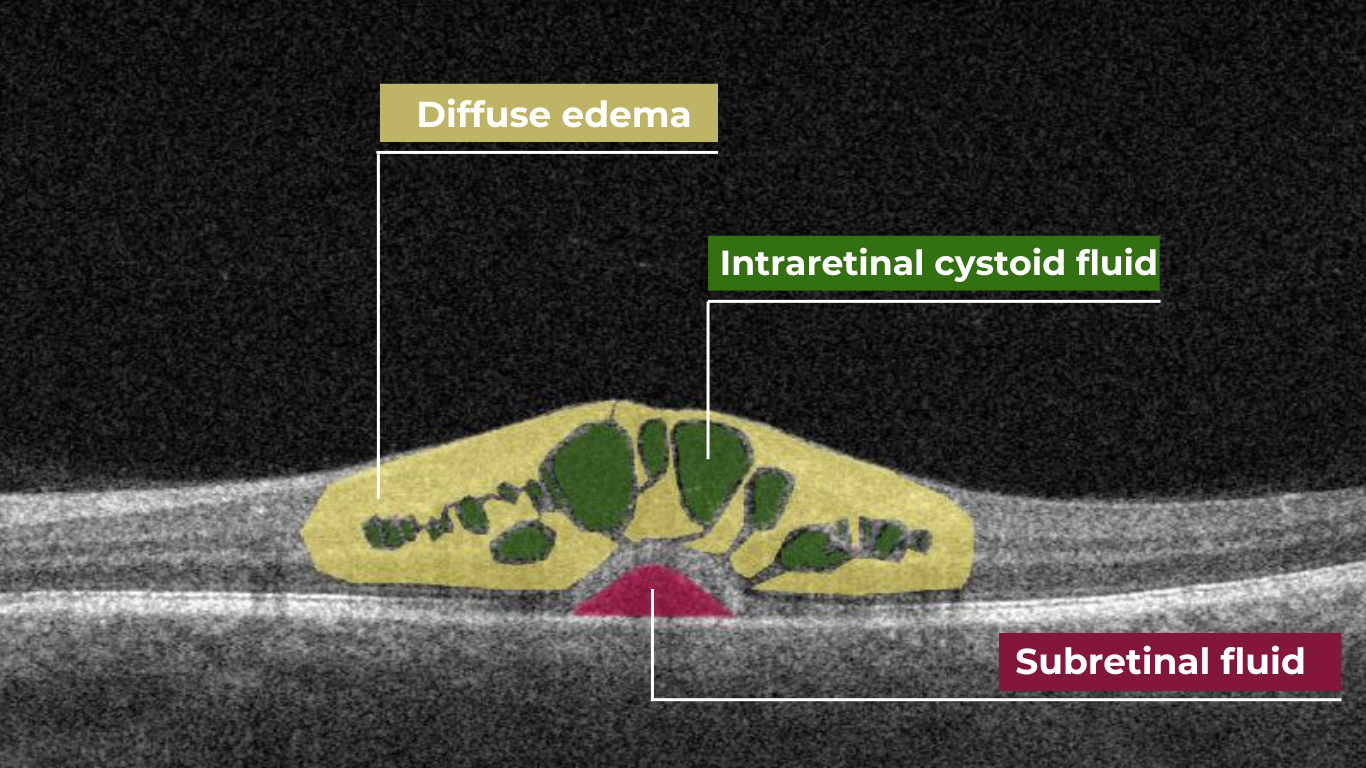
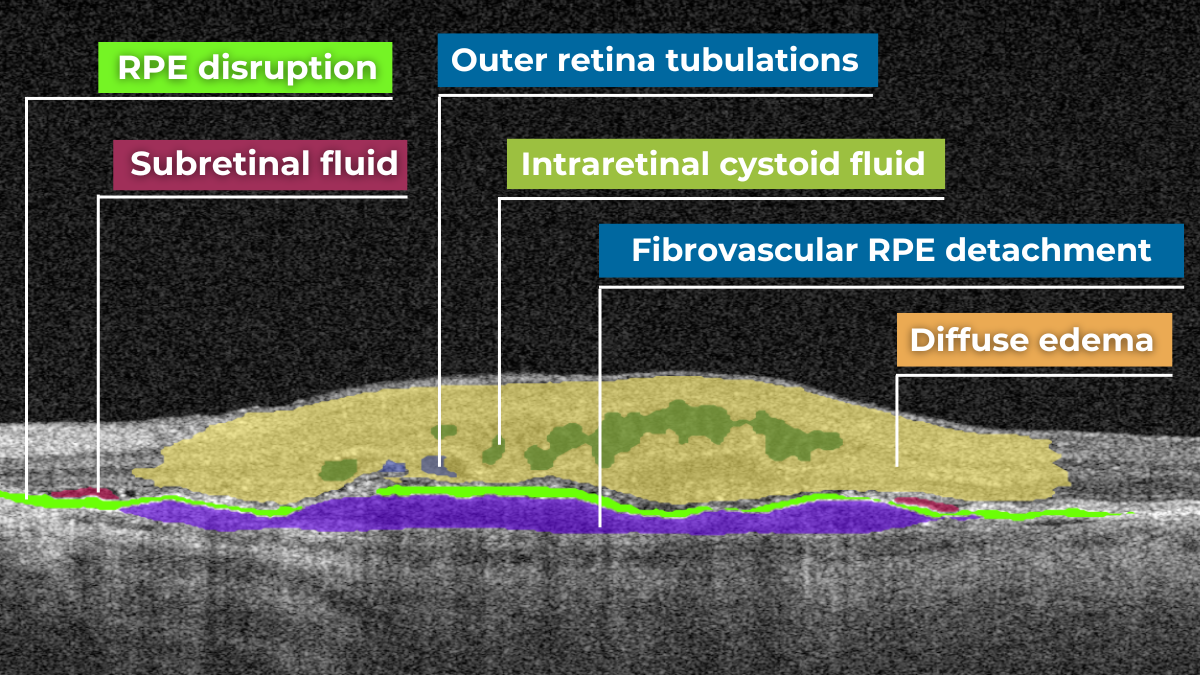
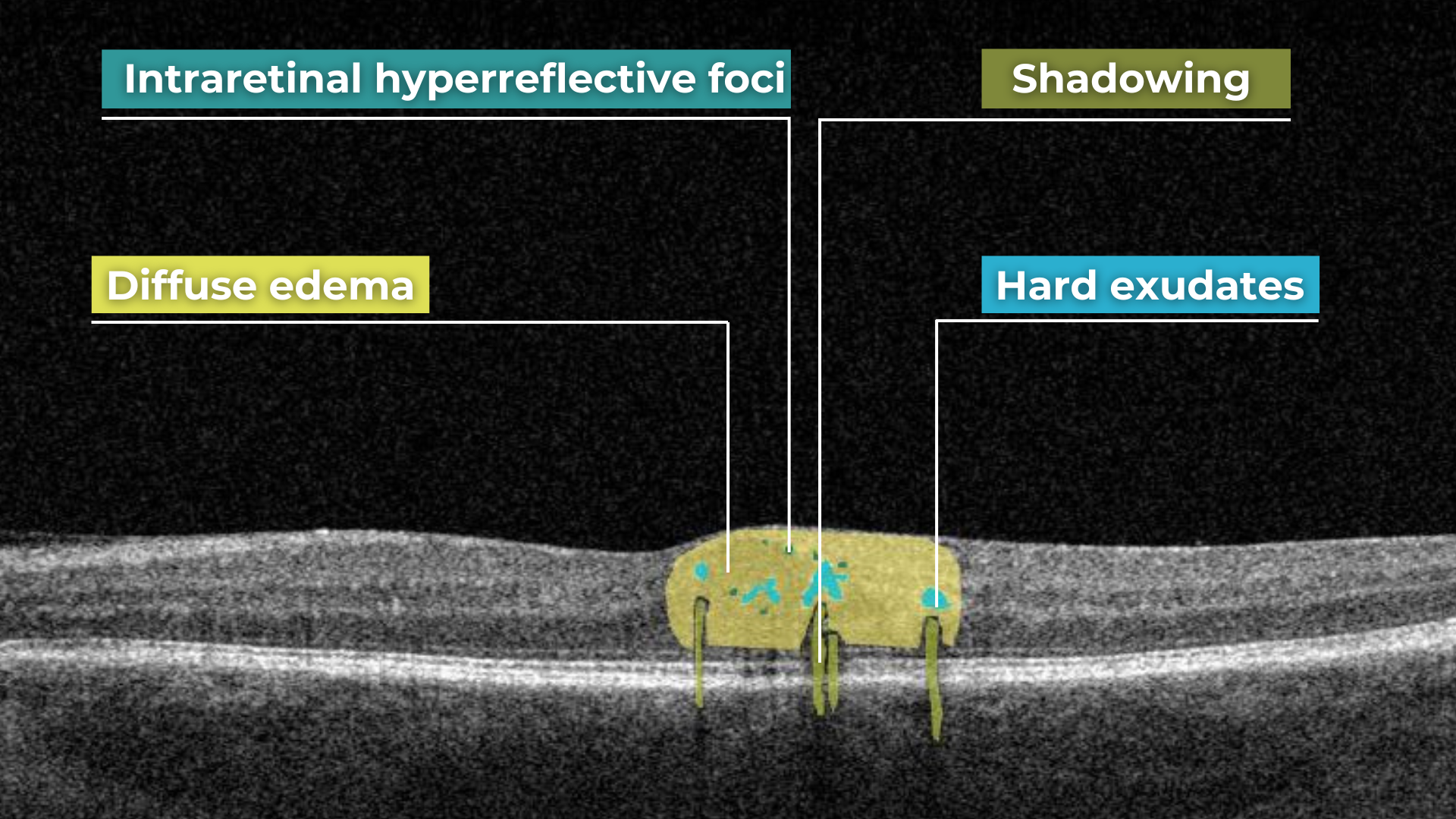
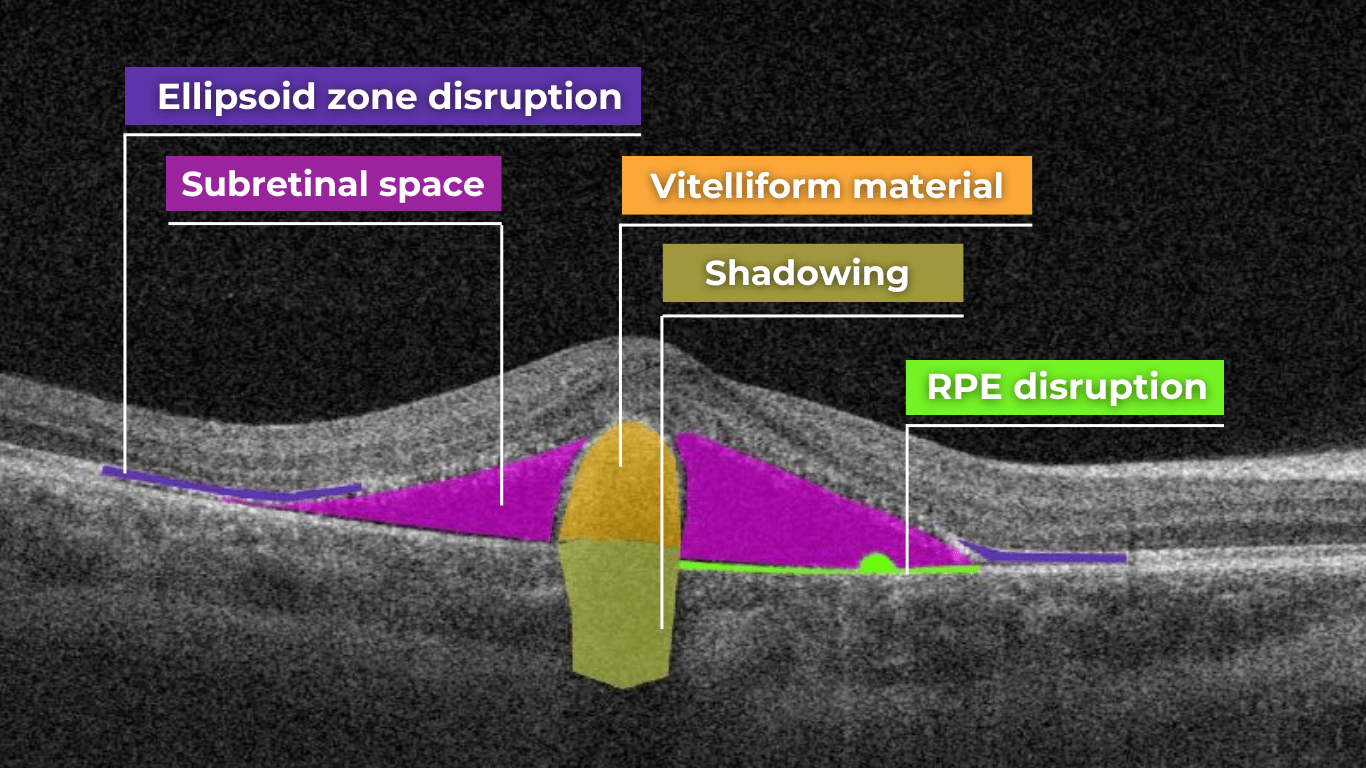
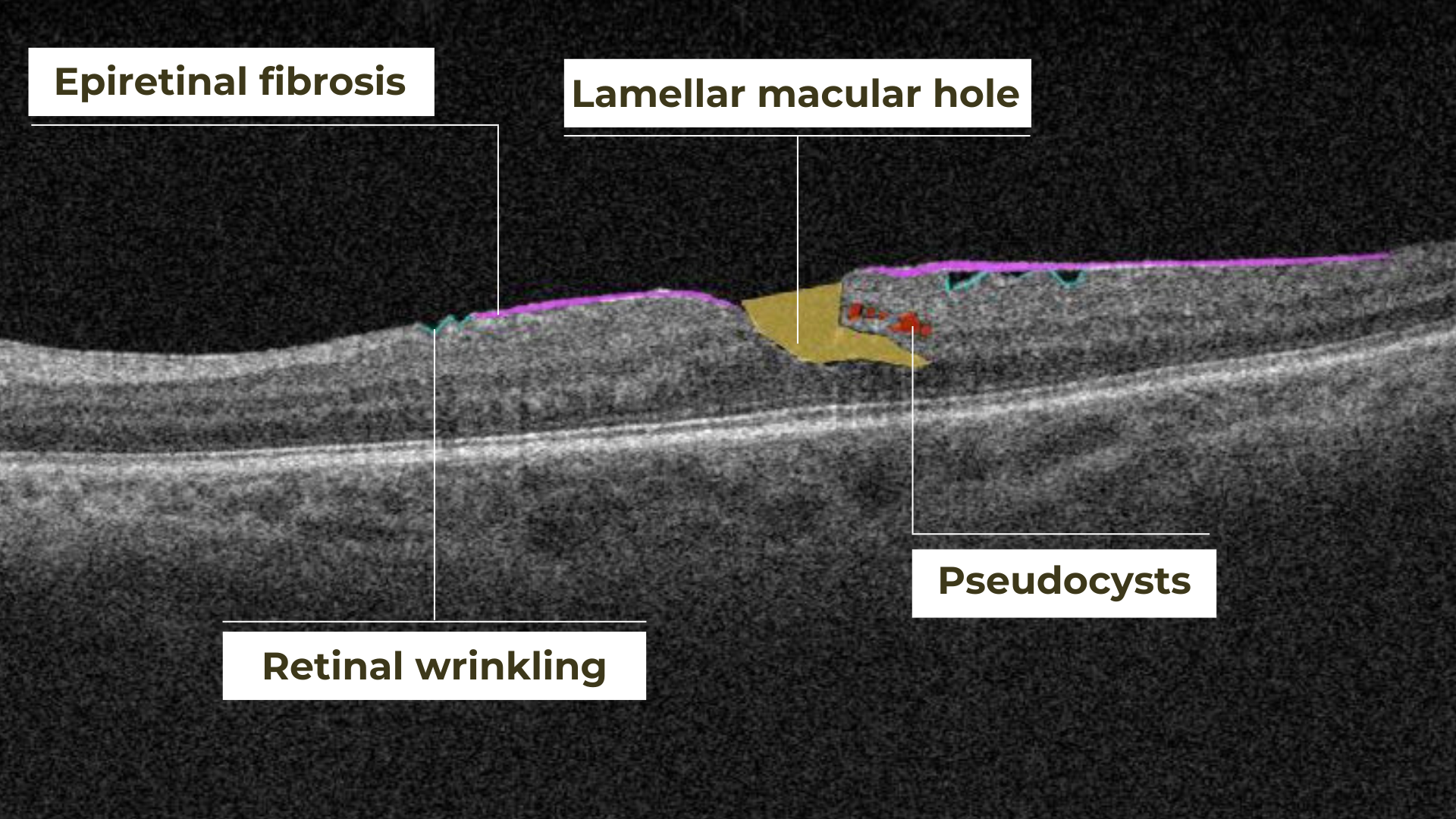
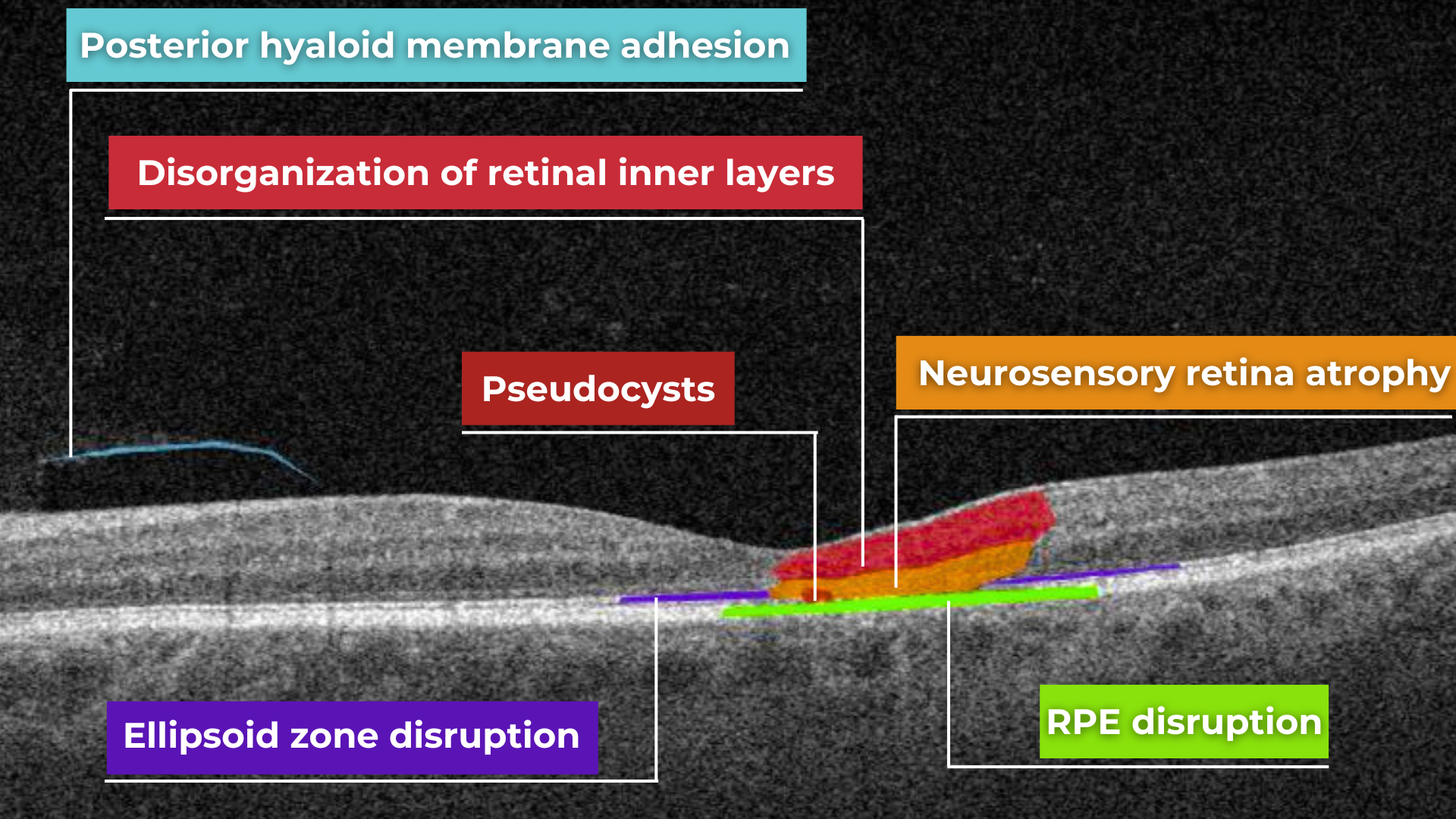
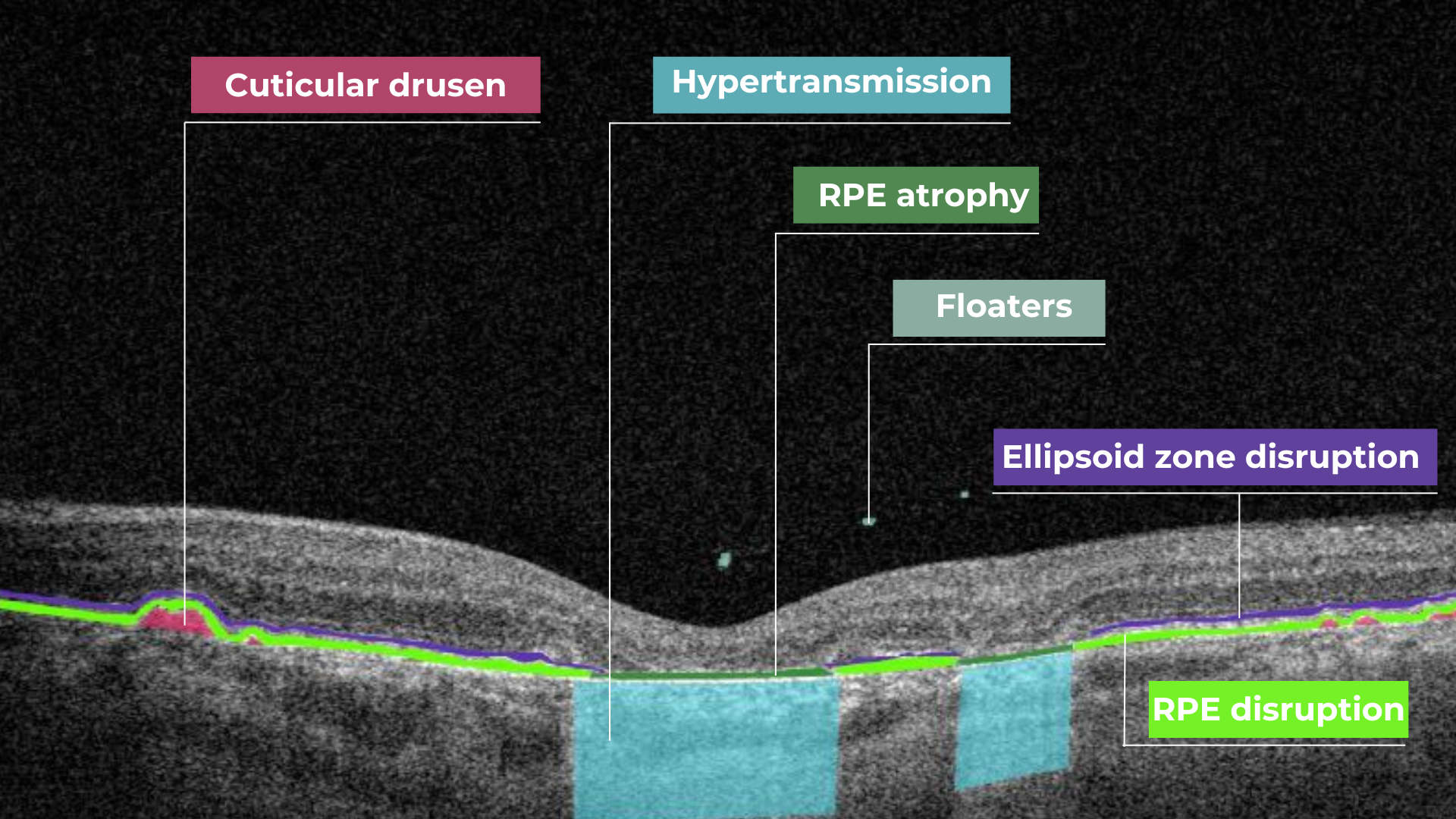 Hypertransmission on OCT
Hypertransmission on OCT