
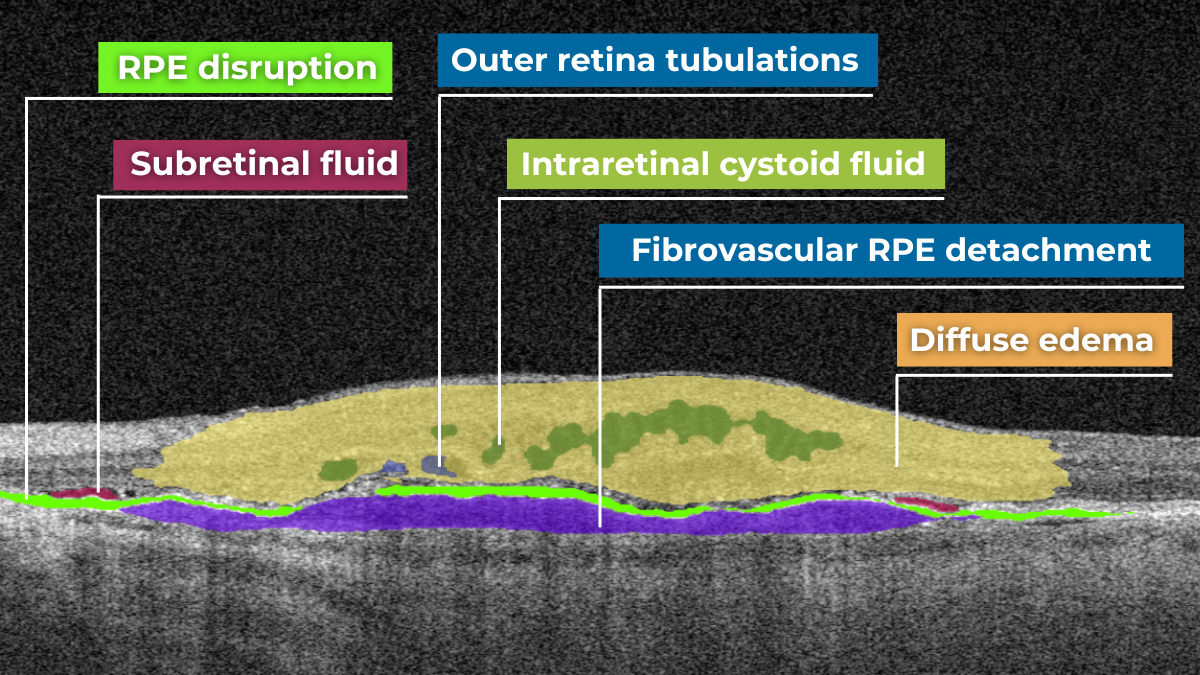











 Hypertransmission on OCT
Hypertransmission on OCT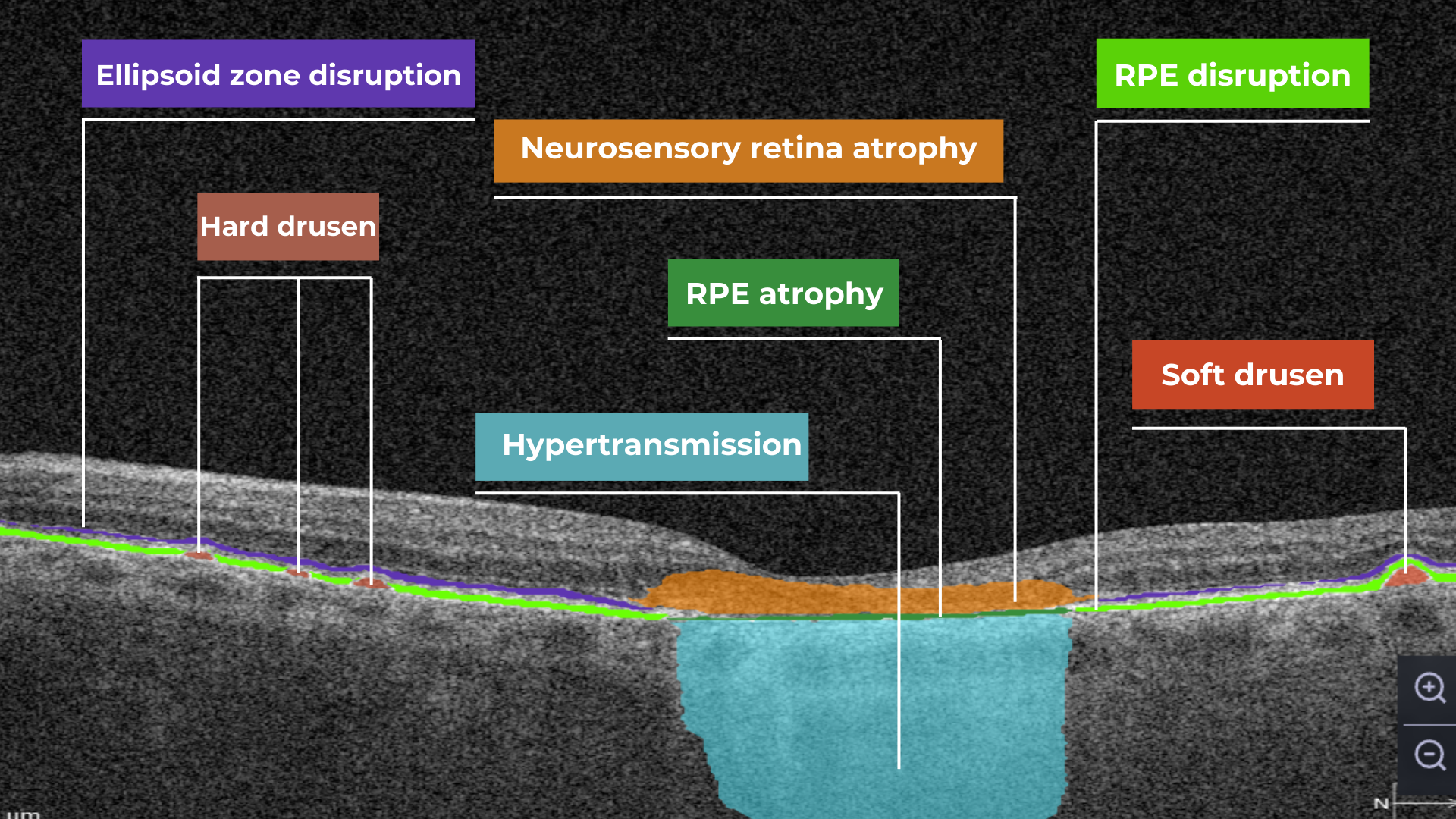



















{kind=link}
In conclusion, Altris AI has built its platform with a strong commitment to ethical AI principles, ensuring patient data protection, transparency, and compliance with global regulations like GDPR HIPAA, EU AI Act. The system is designed to support, not replace, eye care professionals by enhancing diagnostic accuracy and improving early detection of diseases. By emphasizing machine training ethics, patient-related rights, and the usability of their AI tool, Altris AI fosters trust in healthcare technology while maintaining high standards of transparency, accountability, and human oversight in medical decision-making.
Featured This month
-
AI for Decision Support with OCT: “Altris AI Gave Me More Certainty in My Clinical Decisions”
 Maria Martynova
2 minutes
Maria Martynova
2 minutesAI for Decision Support with OCT: An Interview with Clara Pereira, Optometrist from Franco Oculista
About Franco Oculista Optometry in Portugal.
Franco Oculista is the optometry center with a 70-year-old history: its roots date back to the mid-1950s in Luanda, where it was founded by Gonçalo Viana Franco. Having left behind a career in pharmacy, Gonçalo pursued his entrepreneurial vision by opening an optician’s bearing his name in the heart of the Angolan capital. Driven by a thirst for knowledge and a deep sense of dedication, he turned his dream into reality. With a commitment to professionalism and a forward-thinking approach, he integrated the most innovative technologies available at the time. This blend of passion, expertise, and innovation established Franco Oculista as a benchmark for quality and excellence in the field. In 1970s, the family returned to Portugal and opened the new FRANCO OCULISTA space on Avenida da Liberdade.
How do Franco Oculista describe their mission?
“Through individualized and segmented service, we seek to respond to the needs of each client. We combine our knowledge with the most sophisticated technical equipment and choose quality and reliable brands. We prioritize the evolution of our services and, for this reason, we work daily to satisfy and retain our customers with the utmost professionalism.”

Clara Pereira is one of the optometrists at Franco Oculista and has been an optometrist for nearly two decades. Based in a private clinic in Portugal, she brings years of experience and calm confidence to her consultations. We talked with her to learn how her clinical practice has evolved, particularly since integrating OCT and, more recently, Altris AI – AI for Decision Support with OCT.
Altris AI: Clara, can you tell us a bit about your daily work?
Clara: “Of course. I’ve been working as an optometrist for 19 years now. My practice is quite comprehensive—I assess refractive status, binocular vision, check the anterior segment with a slit lamp, measure intraocular pressure, and always examine the fundus.
Clara: “In Portugal, we face limitations. We’re not allowed to prescribe medication or perform cycloplegia, so imaging becomes crucial. I rely heavily on fundus photography and OCT to guide referrals and detect early pathology.”

Altris AI: How central is OCT diagnostics to your workflow?
Clara: “OCT is substantial. I perform an OCT exam on nearly every patient, on average, eight OCT exams per day. It’s an essential part of how I gather information. With just one scan, I can learn so much about eye health.”Altris AI: What kind of conditions do you encounter most frequently?
Clara: “The most common diagnosis is epiretinal membrane—fibrosis. But I also manage patients with macular degeneration and other retinal pathologies. Having the right tools is key.”Altris AI: And what OCT features do you use the most?
Clara: “I regularly use the Retina, Glaucoma, and Macula maps. But if I had to choose one, the Retina Map gives me the most complete picture. It’s become my go-to.”Altris AI: You’ve recently started using Altris AI. What has that experience been like?
Clara: “At first, I didn’t know much about it. But when Optometron introduced Altris AI to me—a company I trust—I didn’t hesitate. And I’m glad I didn’t. From the beginning, it felt like a natural extension of my clinical reasoning.Clara: “Altris AI gives me an extra layer of certainty. It helps me extract more from the OCT images. I usually interpret the scan myself first, and then I run it through the platform. That way, I validate my thinking while also learning something new.”
Altris AI: Have any standout cases where Altris AI made a difference?
Clara: “Yes. I’ve had a few. One was a case of advanced macular degeneration, in which the AI visualization really helped me explain the condition to the patient. Another was using anterior segment maps for fitting scleral lenses—Altris was incredibly useful there, too. I do a lot of specialty lens fittings, so that was a big advantage.”
Altris AI: Would you recommend Altris AI to your colleagues?
Clara: “I would recommend Altris AI to my colleagues. For me, it’s about more than just the diagnosis. It’s about feeling confident that I’m seeing everything clearly and giving my patients the best care possible. Altris AI helps me do exactly that.”
Why This Matters: Altris AI in Real Practice
Clara’s story reflects the real value of AI in optometry—not as a replacement for clinical judgment, but as a powerful companion. With every OCT scan, she strengthens her expertise, improves diagnostic accuracy, and gives her patients the reassurance they deserve.
Whether identifying early signs of fibrosis, supporting complex scleral lens fittings, or acting as a second opinion, Altris AI seamlessly fits into the modern optometrist’s workflow, making every scan more meaningful.
AI for Decision Support with OCT: Transforming Retinal Diagnostics
Artificial Intelligence (AI) is revolutionizing the field of ophthalmology, particularly through its integration with Optical Coherence Tomography (OCT). OCT is a non-invasive imaging technique that captures high-resolution cross-sectional images of the retina, enabling early detection and monitoring of various ocular conditions. However, interpreting these scans requires time, expertise, and consistency—factors that AI-based decision support systems are uniquely positioned to enhance.
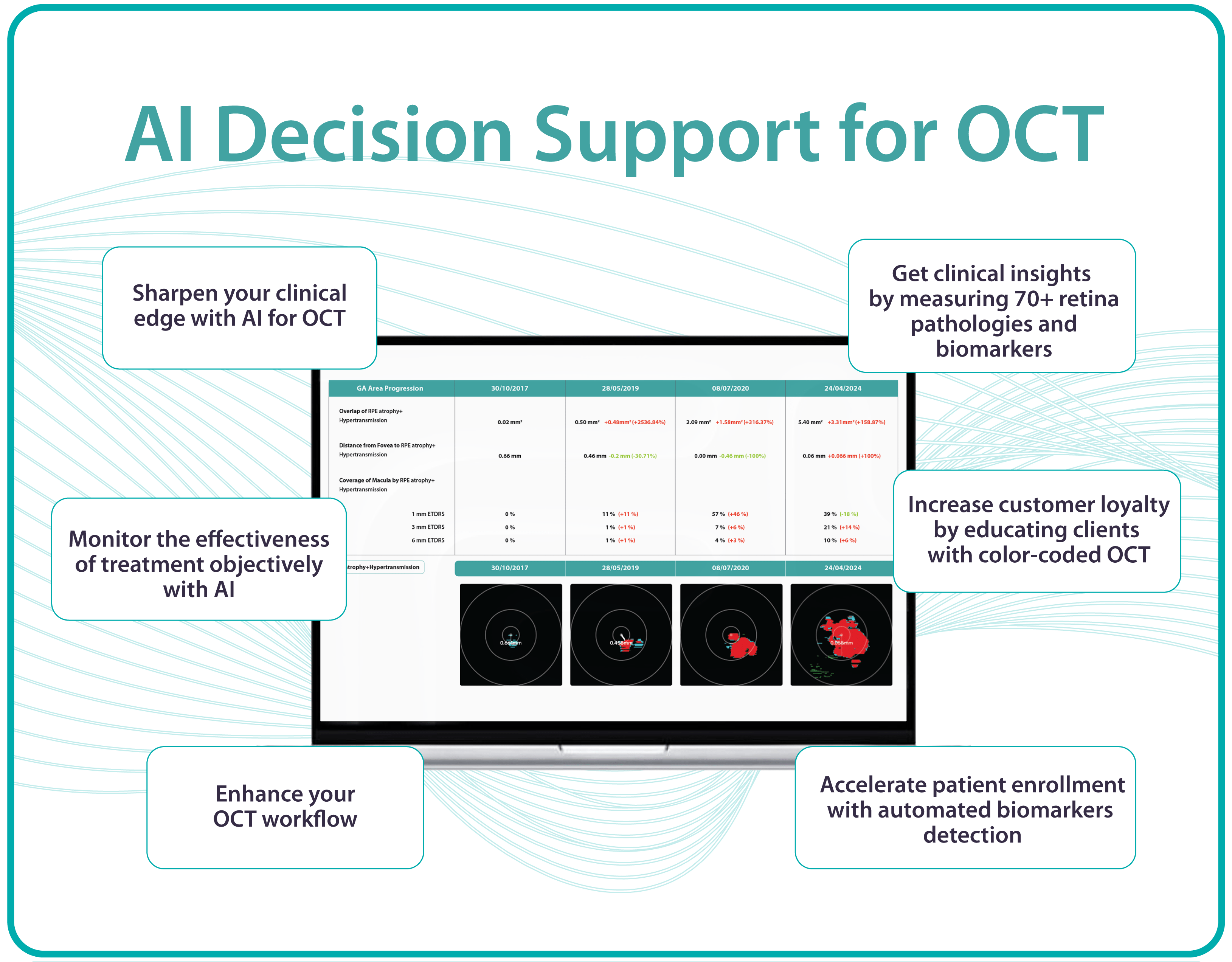
Altris AI (AI for OCT decision support platform) analyzes thousands of data points across B-scans, automatically detecting retinal pathologies, quantifying biomarkers, and identifying patterns that may be subtle or overlooked by the human eye. By providing objective, standardized assessments, Altris AI reduces diagnostic variability and improves clinical accuracy, especially in busy or high-volume practices.
For optometrists and ophthalmologists, AI acts as a second opinion, flagging early signs of diseases such as age-related macular degeneration (AMD), diabetic retinopathy, and glaucoma. It streamlines workflows by highlighting areas of concern, prioritizing cases that require urgent attention, and offering visual explanations that are easy to communicate to patients.
Moreover, Altris AI enableS longitudinal tracking of pathology progression. By comparing OCT scans over time ( even from various OCT devices), clinicians can monitor subtle changes in drusen volume, retinal thickness, supporting timely clinical decisions and tailored treatment strategies. The integration of AI into OCT interpretation not only enhances diagnostic confidence but also supports evidence-based care, early intervention, and improved patient outcomes. As AI continues to evolve, it will play a vital role in advancing precision medicine in ophthalmology, empowering eye care professionals with tools that are fast, reliable, and scalable.

In essence, AI for OCT decision support is not replacing clinical expertise; it is augmenting it, elevating the standard of care through speed, accuracy, and actionable insights.
-
Best AI for OCT: 10 Essential Features Your Platform Must Have
Maria Martynova
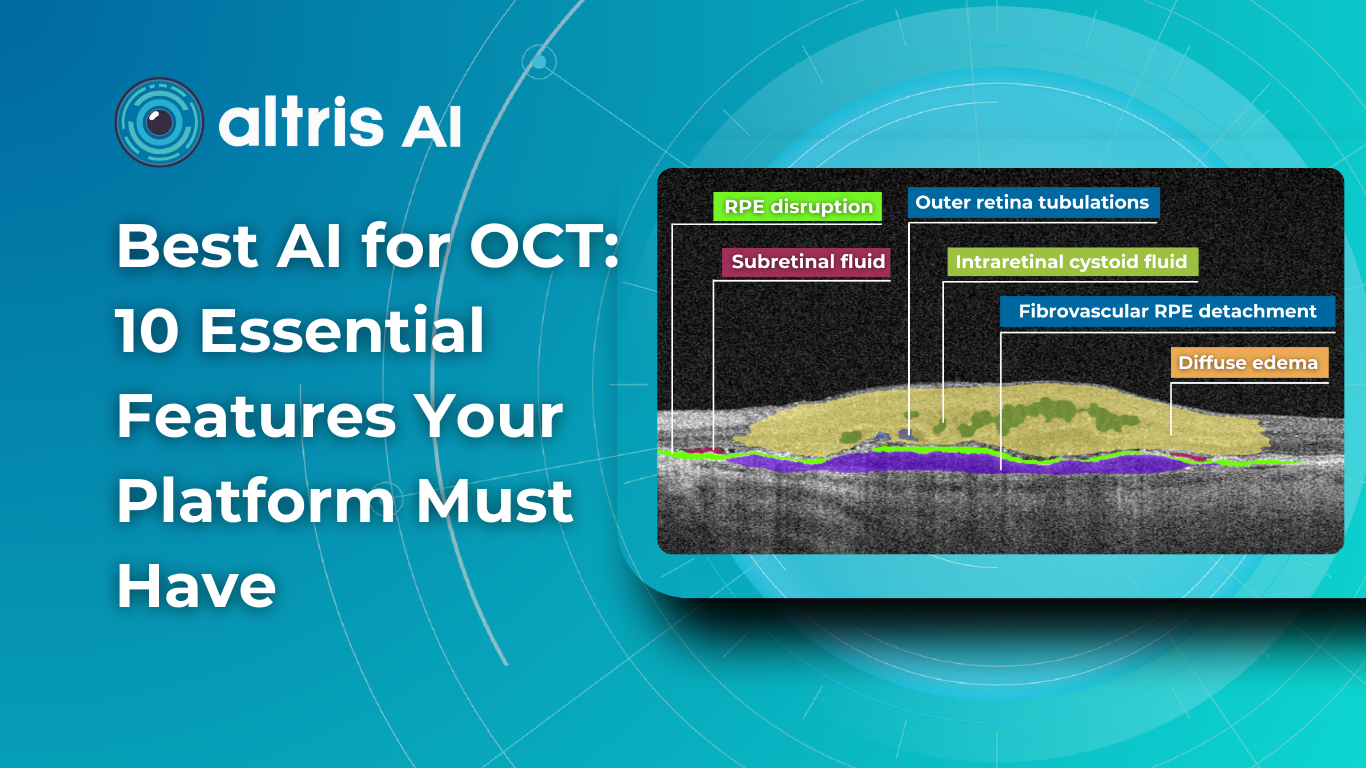
8 min.Best AI for OCT: 10 Essential Features Your Platform Must Have
So you’ve decided to trial AI for OCT analysis and wondering how to choose among all the available platforms. To save you some time, we’ve collected 10 most essential criteria according to which you can assess all existing AI platforms. Using this criteria you will be able to make an informed and rational choice.
As an ophthalmologist, I am interested in finding innovative and modern approaches that could help me to enhance the workflow and improve patient outcome as a result.Analyzing various platforms, I realized that these 10 criteria are crucial for the right choice.
1. Regulatory Compliance and Clinical Validation
In healthcare, safety is always first. Regulatory approval and clinical validation are essential for AI-powered platforms for OCT scan analysis.
The best AI OCT platforms should meet regulatory standards set by authorities such as the FDA, HIPAA, CE, and ISO.
Adhering to regulatory guidelines enhances credibility and fosters trust among healthcare professionals. Check if the AI for OCT analysis tool has all these certificates in place and if they are valid.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
2.Wide range of biomarkers and pathologies detected
Some AI for OCT platforms concentrate on certain pathologies, like Age-Related Macular Degeneration (AMD) or Diabetic Retinopathy, because of the prevalence of these conditions among the population. It mostly means that eye care specialists must know in advance that they are dealing with the AMD patient to find the proof of AMD on the OCT.
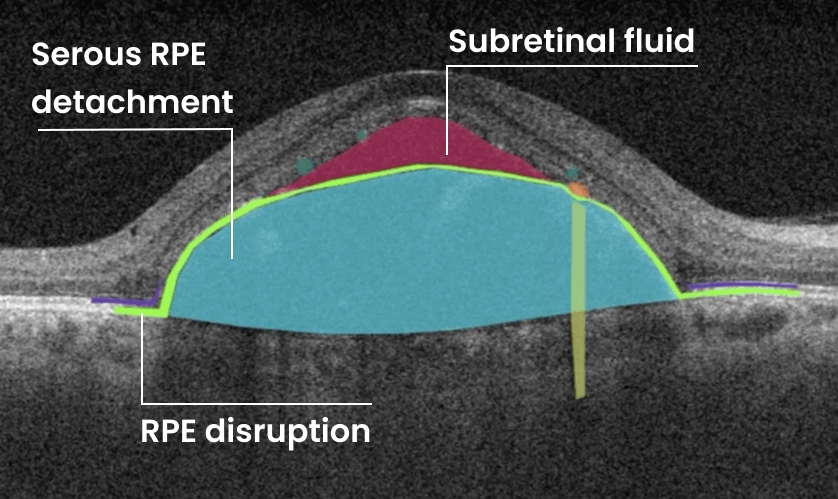
The best AI for OCT tools should have a wide variety of biomarkers and pathologies, including rare ones that cannot be seen daily in clinical practice, such as central retinal vein and artery occlusions, vitelliform dystrophy, macular telangiectasia and others. Altris AI, the leader of OCT for AI analysis, detects 74 biomarkers and pathologies as of today.

3.Cloud-Based Data Management and Accessibility
To ensure seamless integration into clinical workflows, the AI OCT platform should offer cloud-based data management and accessibility. Cloud storage allows for easy retrieval of patient records, remote consultations, and multi-location access. Secure cloud computing also enhances collaboration between ophthalmologists, optometrists, and researchers by enabling data sharing while maintaining compliance with data privacy regulations such as HIPAA and GDPR.
Many clinics have strict policies regarding patient data storage as well: it is crucial that the data is stored on the servers in the region of operation. If the clinic is in EU, the data should be stored in the EU.
4.Real-world usage by eye care specialists
When choosing the best AI for OCT analysis, real-world usage by eye care specialists is the most critical factor. Advanced algorithms and high accuracy metrics mean little if the AI is not seamlessly integrated into clinical workflows and actively used by optometrists and ophthalmologists. There are thousands of research models available, but when it comes to the implementation, most of them are not available to ECPs.
Eye care professionals are not IT specialists. They require AI that is intuitive, fast, and reliable. If a system disrupts their workflow, generates excessive false alerts, or lacks clear explanations for its findings, adoption rates will be low—even if the technology itself is powerful. The best AI solutions are those that specialists trust and rely on daily to enhance diagnostic accuracy, streamline patient management, and support decision-making.
Moreover, real usage generates valuable feedback that continuously improves the AI. Systems actively used in clinical settings undergo rapid validation, refinement, and adaptation to diverse patient populations. This real-world data is far more meaningful than isolated test results in controlled environments.
5. Customizable Reporting and Visualization Tools
Reports are the result of the whole AI for OCT scan analysis that is why customizable and comprehensive reports are a must.
A high-quality AI OCT platform must offer customizable reporting and visualization tools. Clinicians should be able to adjust parameters, select specific data points, and generate detailed reports tailored to individual patient needs.
Heatmaps, 3D reconstructions, and trend analysis graphs should be available to help visualize disease progression. These tools improve the interpretability of AI-generated insights and facilitate patient education.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
6.AI for Early Glaucoma Detection
Glaucoma is a leading cause of irreversible blindness, and since OCT is widely used to assess the retinal nerve fiber layer (RNFL), Ganglion Cell Complex ( GCC), optic nerve head (ONH), AI can significantly enhance early detection and risk assessment.
Therefore, the best AI for OCT analysis tools have an AI for early glaucoma detection module available to assess the risk of glaucoma especially at the early stage. Moreover, tracking the progression of glaucoma with the help of AI should also be available for eye care specialists.
Clear and bright notifications about glaucoma risk are also vital for making AI glaucoma modules easy to use. AI can provide proactive insights that enable early intervention and personalized treatment plans
7.User – Friendly Interface and Intuitive Workflow Integration
A well-designed AI OCT platform should feature a user-friendly interface that integrates seamlessly into existing clinical workflows.
It means that even non-tech-savvy eye care specialists should be able to navigate it effortlessly.
The interface should be intuitive, reducing the learning curve for healthcare providers. Features such as automated scan interpretation, voice command functionality, and guided step-by-step analysis can enhance usability and efficiency.
8.Integration with Electronic Health Records (EHRs)
For a seamless clinical experience, the AI OCT platform should integrate with existing electronic health record (EHR) systems. Automated data synchronization between AI analysis and patient records enhances workflow efficiency and reduces administrative burden. This feature enables real-time updates, streamlined documentation, and easy access to past diagnostic reports.
9. Universal AI solutions compatible with all OCT devices
Uf you want to use AI to analyze OCT, this AI should be trained on data received from various OCT devices and therefore should be applicable with various OCT devices. A vendor-neutral AI tool for OCT analysis provides unmatched advantages over proprietary solutions tied to specific hardware. By working seamlessly with multiple OCT devices, it eliminates the need for costly equipment upgrades and ensures broader accessibility across clinics and hospitals.
This approach also fosters greater innovation, allowing AI models to continuously improve based on diverse datasets rather than being limited to a single manufacturer’s ecosystem. Vendor-neutral solutions integrate effortlessly into existing workflows, reducing training time and boosting efficiency. Clinicians benefit from unbiased, adaptable technology that prioritizes patient outcomes rather than locking users into restrictive ecosystems.
10. Cost-Effectiveness and Accessibility
To maximize its impact, an AI-powered OCT platform should be cost-effective and accessible to a wide range of healthcare providers. Affordable pricing models, including subscription-based or pay-per-use plans, can make AI technology available to smaller clinics and developing regions. Accessibility ensures that AI-driven OCT analysis benefits as many patients as possible, improving global eye health outcomes.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
Conclusion
What is the best AI for OCT scan analysis? The best AI for OCT must be a comprehensive, intelligent, and adaptable platform that enhances diagnostic accuracy, streamlines clinical workflows, and supports proactive eye care. Key features such as high-accuracy automated analysis, multi-modal imaging integration, real-time decision support, cloud-based data management, interoperability, and explainable AI decision-making are crucial for an effective OCT AI system. By incorporating these attributes, AI-driven OCT platforms can revolutionize ophthalmology, enabling early disease detection, personalized treatment planning, and improved patient outcomes. As AI technology continues to advance, its integration with OCT will play an increasingly vital role in shaping the future of eye care.
popular Posted
-
AI for Decision Support with OCT: “Altris AI Gave Me More Certainty in My Clinical Decisions”
 Maria Martynova
2 minutes
Maria Martynova
2 minutesAI for Decision Support with OCT: An Interview with Clara Pereira, Optometrist from Franco Oculista
About Franco Oculista Optometry in Portugal.
Franco Oculista is the optometry center with a 70-year-old history: its roots date back to the mid-1950s in Luanda, where it was founded by Gonçalo Viana Franco. Having left behind a career in pharmacy, Gonçalo pursued his entrepreneurial vision by opening an optician’s bearing his name in the heart of the Angolan capital. Driven by a thirst for knowledge and a deep sense of dedication, he turned his dream into reality. With a commitment to professionalism and a forward-thinking approach, he integrated the most innovative technologies available at the time. This blend of passion, expertise, and innovation established Franco Oculista as a benchmark for quality and excellence in the field. In 1970s, the family returned to Portugal and opened the new FRANCO OCULISTA space on Avenida da Liberdade.
How do Franco Oculista describe their mission?
“Through individualized and segmented service, we seek to respond to the needs of each client. We combine our knowledge with the most sophisticated technical equipment and choose quality and reliable brands. We prioritize the evolution of our services and, for this reason, we work daily to satisfy and retain our customers with the utmost professionalism.”
Clara Pereira is one of the optometrists at Franco Oculista and has been an optometrist for nearly two decades. Based in a private clinic in Portugal, she brings years of experience and calm confidence to her consultations. We talked with her to learn how her clinical practice has evolved, particularly since integrating OCT and, more recently, Altris AI – AI for Decision Support with OCT.
Altris AI: Clara, can you tell us a bit about your daily work?
Clara: “Of course. I’ve been working as an optometrist for 19 years now. My practice is quite comprehensive—I assess refractive status, binocular vision, check the anterior segment with a slit lamp, measure intraocular pressure, and always examine the fundus.
Clara: “In Portugal, we face limitations. We’re not allowed to prescribe medication or perform cycloplegia, so imaging becomes crucial. I rely heavily on fundus photography and OCT to guide referrals and detect early pathology.”
Altris AI: How central is OCT diagnostics to your workflow?
Clara: “OCT is substantial. I perform an OCT exam on nearly every patient, on average, eight OCT exams per day. It’s an essential part of how I gather information. With just one scan, I can learn so much about eye health.”Altris AI: What kind of conditions do you encounter most frequently?
Clara: “The most common diagnosis is epiretinal membrane—fibrosis. But I also manage patients with macular degeneration and other retinal pathologies. Having the right tools is key.”Altris AI: And what OCT features do you use the most?
Clara: “I regularly use the Retina, Glaucoma, and Macula maps. But if I had to choose one, the Retina Map gives me the most complete picture. It’s become my go-to.”Altris AI: You’ve recently started using Altris AI. What has that experience been like?
Clara: “At first, I didn’t know much about it. But when Optometron introduced Altris AI to me—a company I trust—I didn’t hesitate. And I’m glad I didn’t. From the beginning, it felt like a natural extension of my clinical reasoning.Clara: “Altris AI gives me an extra layer of certainty. It helps me extract more from the OCT images. I usually interpret the scan myself first, and then I run it through the platform. That way, I validate my thinking while also learning something new.”
Altris AI: Have any standout cases where Altris AI made a difference?
Clara: “Yes. I’ve had a few. One was a case of advanced macular degeneration, in which the AI visualization really helped me explain the condition to the patient. Another was using anterior segment maps for fitting scleral lenses—Altris was incredibly useful there, too. I do a lot of specialty lens fittings, so that was a big advantage.”
Altris AI: Would you recommend Altris AI to your colleagues?
Clara: “I would recommend Altris AI to my colleagues. For me, it’s about more than just the diagnosis. It’s about feeling confident that I’m seeing everything clearly and giving my patients the best care possible. Altris AI helps me do exactly that.”
Why This Matters: Altris AI in Real Practice
Clara’s story reflects the real value of AI in optometry—not as a replacement for clinical judgment, but as a powerful companion. With every OCT scan, she strengthens her expertise, improves diagnostic accuracy, and gives her patients the reassurance they deserve.
Whether identifying early signs of fibrosis, supporting complex scleral lens fittings, or acting as a second opinion, Altris AI seamlessly fits into the modern optometrist’s workflow, making every scan more meaningful.
AI for Decision Support with OCT: Transforming Retinal Diagnostics
Artificial Intelligence (AI) is revolutionizing the field of ophthalmology, particularly through its integration with Optical Coherence Tomography (OCT). OCT is a non-invasive imaging technique that captures high-resolution cross-sectional images of the retina, enabling early detection and monitoring of various ocular conditions. However, interpreting these scans requires time, expertise, and consistency—factors that AI-based decision support systems are uniquely positioned to enhance.
Altris AI (AI for OCT decision support platform) analyzes thousands of data points across B-scans, automatically detecting retinal pathologies, quantifying biomarkers, and identifying patterns that may be subtle or overlooked by the human eye. By providing objective, standardized assessments, Altris AI reduces diagnostic variability and improves clinical accuracy, especially in busy or high-volume practices.
For optometrists and ophthalmologists, AI acts as a second opinion, flagging early signs of diseases such as age-related macular degeneration (AMD), diabetic retinopathy, and glaucoma. It streamlines workflows by highlighting areas of concern, prioritizing cases that require urgent attention, and offering visual explanations that are easy to communicate to patients.
Moreover, Altris AI enableS longitudinal tracking of pathology progression. By comparing OCT scans over time ( even from various OCT devices), clinicians can monitor subtle changes in drusen volume, retinal thickness, supporting timely clinical decisions and tailored treatment strategies. The integration of AI into OCT interpretation not only enhances diagnostic confidence but also supports evidence-based care, early intervention, and improved patient outcomes. As AI continues to evolve, it will play a vital role in advancing precision medicine in ophthalmology, empowering eye care professionals with tools that are fast, reliable, and scalable.
In essence, AI for OCT decision support is not replacing clinical expertise; it is augmenting it, elevating the standard of care through speed, accuracy, and actionable insights.
-
Best AI for OCT: 10 Essential Features Your Platform Must Have
Maria Martynova
8 min.Best AI for OCT: 10 Essential Features Your Platform Must Have
So you’ve decided to trial AI for OCT analysis and wondering how to choose among all the available platforms. To save you some time, we’ve collected 10 most essential criteria according to which you can assess all existing AI platforms. Using this criteria you will be able to make an informed and rational choice.
As an ophthalmologist, I am interested in finding innovative and modern approaches that could help me to enhance the workflow and improve patient outcome as a result.Analyzing various platforms, I realized that these 10 criteria are crucial for the right choice.
1. Regulatory Compliance and Clinical Validation
In healthcare, safety is always first. Regulatory approval and clinical validation are essential for AI-powered platforms for OCT scan analysis.
The best AI OCT platforms should meet regulatory standards set by authorities such as the FDA, HIPAA, CE, and ISO.
Adhering to regulatory guidelines enhances credibility and fosters trust among healthcare professionals. Check if the AI for OCT analysis tool has all these certificates in place and if they are valid.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
2.Wide range of biomarkers and pathologies detected
Some AI for OCT platforms concentrate on certain pathologies, like Age-Related Macular Degeneration (AMD) or Diabetic Retinopathy, because of the prevalence of these conditions among the population. It mostly means that eye care specialists must know in advance that they are dealing with the AMD patient to find the proof of AMD on the OCT.
The best AI for OCT tools should have a wide variety of biomarkers and pathologies, including rare ones that cannot be seen daily in clinical practice, such as central retinal vein and artery occlusions, vitelliform dystrophy, macular telangiectasia and others. Altris AI, the leader of OCT for AI analysis, detects 74 biomarkers and pathologies as of today.
3.Cloud-Based Data Management and Accessibility
To ensure seamless integration into clinical workflows, the AI OCT platform should offer cloud-based data management and accessibility. Cloud storage allows for easy retrieval of patient records, remote consultations, and multi-location access. Secure cloud computing also enhances collaboration between ophthalmologists, optometrists, and researchers by enabling data sharing while maintaining compliance with data privacy regulations such as HIPAA and GDPR.
Many clinics have strict policies regarding patient data storage as well: it is crucial that the data is stored on the servers in the region of operation. If the clinic is in EU, the data should be stored in the EU.
4.Real-world usage by eye care specialists
When choosing the best AI for OCT analysis, real-world usage by eye care specialists is the most critical factor. Advanced algorithms and high accuracy metrics mean little if the AI is not seamlessly integrated into clinical workflows and actively used by optometrists and ophthalmologists. There are thousands of research models available, but when it comes to the implementation, most of them are not available to ECPs.
Eye care professionals are not IT specialists. They require AI that is intuitive, fast, and reliable. If a system disrupts their workflow, generates excessive false alerts, or lacks clear explanations for its findings, adoption rates will be low—even if the technology itself is powerful. The best AI solutions are those that specialists trust and rely on daily to enhance diagnostic accuracy, streamline patient management, and support decision-making.
Moreover, real usage generates valuable feedback that continuously improves the AI. Systems actively used in clinical settings undergo rapid validation, refinement, and adaptation to diverse patient populations. This real-world data is far more meaningful than isolated test results in controlled environments.
5. Customizable Reporting and Visualization Tools
Reports are the result of the whole AI for OCT scan analysis that is why customizable and comprehensive reports are a must.
A high-quality AI OCT platform must offer customizable reporting and visualization tools. Clinicians should be able to adjust parameters, select specific data points, and generate detailed reports tailored to individual patient needs.
Heatmaps, 3D reconstructions, and trend analysis graphs should be available to help visualize disease progression. These tools improve the interpretability of AI-generated insights and facilitate patient education.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
6.AI for Early Glaucoma Detection
Glaucoma is a leading cause of irreversible blindness, and since OCT is widely used to assess the retinal nerve fiber layer (RNFL), Ganglion Cell Complex ( GCC), optic nerve head (ONH), AI can significantly enhance early detection and risk assessment.
Therefore, the best AI for OCT analysis tools have an AI for early glaucoma detection module available to assess the risk of glaucoma especially at the early stage. Moreover, tracking the progression of glaucoma with the help of AI should also be available for eye care specialists.
Clear and bright notifications about glaucoma risk are also vital for making AI glaucoma modules easy to use. AI can provide proactive insights that enable early intervention and personalized treatment plans
7.User – Friendly Interface and Intuitive Workflow Integration
A well-designed AI OCT platform should feature a user-friendly interface that integrates seamlessly into existing clinical workflows.
It means that even non-tech-savvy eye care specialists should be able to navigate it effortlessly.
The interface should be intuitive, reducing the learning curve for healthcare providers. Features such as automated scan interpretation, voice command functionality, and guided step-by-step analysis can enhance usability and efficiency.
8.Integration with Electronic Health Records (EHRs)
For a seamless clinical experience, the AI OCT platform should integrate with existing electronic health record (EHR) systems. Automated data synchronization between AI analysis and patient records enhances workflow efficiency and reduces administrative burden. This feature enables real-time updates, streamlined documentation, and easy access to past diagnostic reports.
9. Universal AI solutions compatible with all OCT devices
Uf you want to use AI to analyze OCT, this AI should be trained on data received from various OCT devices and therefore should be applicable with various OCT devices. A vendor-neutral AI tool for OCT analysis provides unmatched advantages over proprietary solutions tied to specific hardware. By working seamlessly with multiple OCT devices, it eliminates the need for costly equipment upgrades and ensures broader accessibility across clinics and hospitals.
This approach also fosters greater innovation, allowing AI models to continuously improve based on diverse datasets rather than being limited to a single manufacturer’s ecosystem. Vendor-neutral solutions integrate effortlessly into existing workflows, reducing training time and boosting efficiency. Clinicians benefit from unbiased, adaptable technology that prioritizes patient outcomes rather than locking users into restrictive ecosystems.
10. Cost-Effectiveness and Accessibility
To maximize its impact, an AI-powered OCT platform should be cost-effective and accessible to a wide range of healthcare providers. Affordable pricing models, including subscription-based or pay-per-use plans, can make AI technology available to smaller clinics and developing regions. Accessibility ensures that AI-driven OCT analysis benefits as many patients as possible, improving global eye health outcomes.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
Conclusion
What is the best AI for OCT scan analysis? The best AI for OCT must be a comprehensive, intelligent, and adaptable platform that enhances diagnostic accuracy, streamlines clinical workflows, and supports proactive eye care. Key features such as high-accuracy automated analysis, multi-modal imaging integration, real-time decision support, cloud-based data management, interoperability, and explainable AI decision-making are crucial for an effective OCT AI system. By incorporating these attributes, AI-driven OCT platforms can revolutionize ophthalmology, enabling early disease detection, personalized treatment planning, and improved patient outcomes. As AI technology continues to advance, its integration with OCT will play an increasingly vital role in shaping the future of eye care.
-
Future of Ophthalmology: 2025 Top Trends
Maria Znamenska
13.03.202512 min readFuture of Ophthalmology: 2025 Top Trends
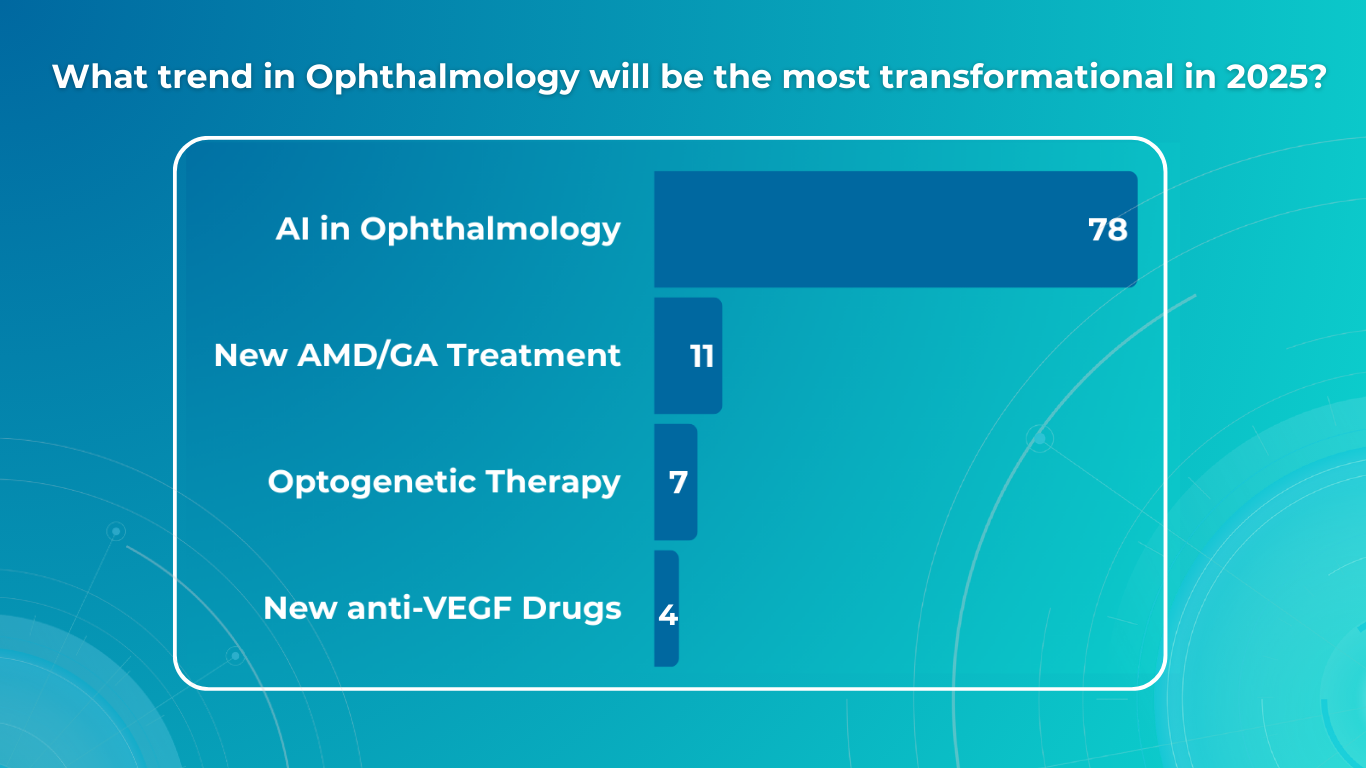
In a recent survey conducted by our team, we asked eye care specialists to identify the most transformative trends in ophthalmology by 2025. The results highlighted several key areas, with artificial intelligence (AI) emerging as the clear frontrunner, cited by 78% of respondents.
However, the survey also underscored the significant impact of optogenetics, novel AMD/GA therapies, and the continuing evolution of anti-VEGF treatments. This article will explore the practical implications of these advancements, providing an overview of how they are poised to reshape diagnosis, treatment, research, and, ultimately, patient outcomes in ophthalmology.
In this article, we will also discuss Oculomics, a very promising field that is gaining momentum.
FDA-cleared AI for OCT analysis
Top AI Technology for Detecting Eye-related Health Risks 2025
Building upon the survey’s findings, we begin with the most prevalent trend: top AI technology for detecting eye-related health risks in 2025

AI in Clinical Eye Care Practice
With the increasing prevalence of conditions like diabetic retinopathy and age-related macular degeneration, there is a growing need for efficient and accurate screening tools. And AI is already valuable for eye-care screening: algorithms can analyze retinal images and OCT scans to identify signs of these diseases, enabling early detection and timely intervention.
AI-powered screening tools can also help identify rare inherited retinal dystrophies, such as Vitelliform dystrophy and Macular telangiectasia type 2. These conditions can be challenging to diagnose, but AI algorithms can analyze retinal images to detect subtle signs that human observers may miss.
AI also starts to play a crucial role in glaucoma management. Early detection of glaucoma demands exceptional precision, as the early signs are often subtle and difficult to detect. Another significant challenge in glaucoma screening is the high rate of false positive referrals, which can lead to unnecessary appointments in secondary care and cause anxiety for patients, yet delayed or missed detection of glaucoma results in irreversible vision loss for millions of people worldwide. So, automated AI-powered glaucoma analysis can offer transformative potential to improve patient outcomes.
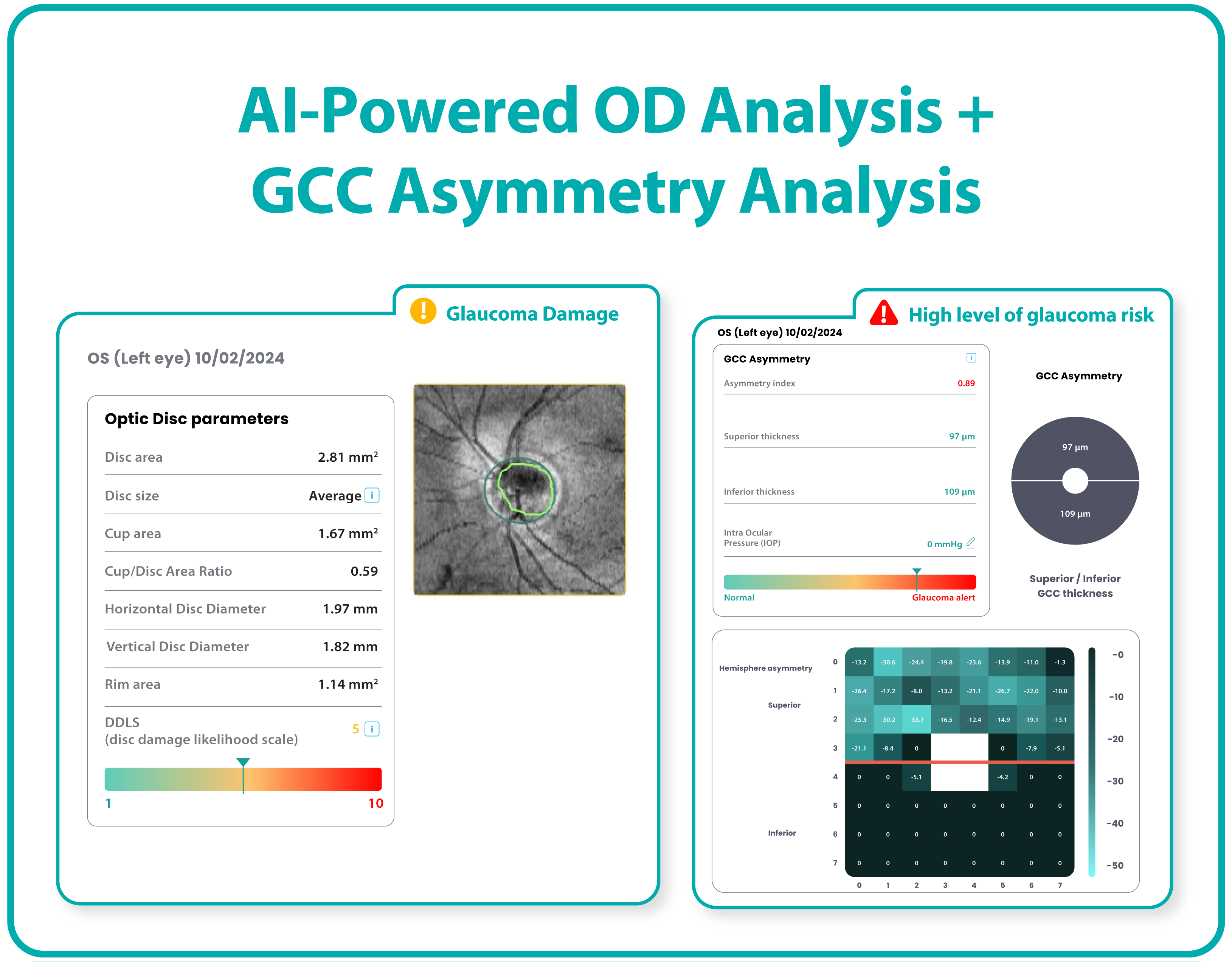
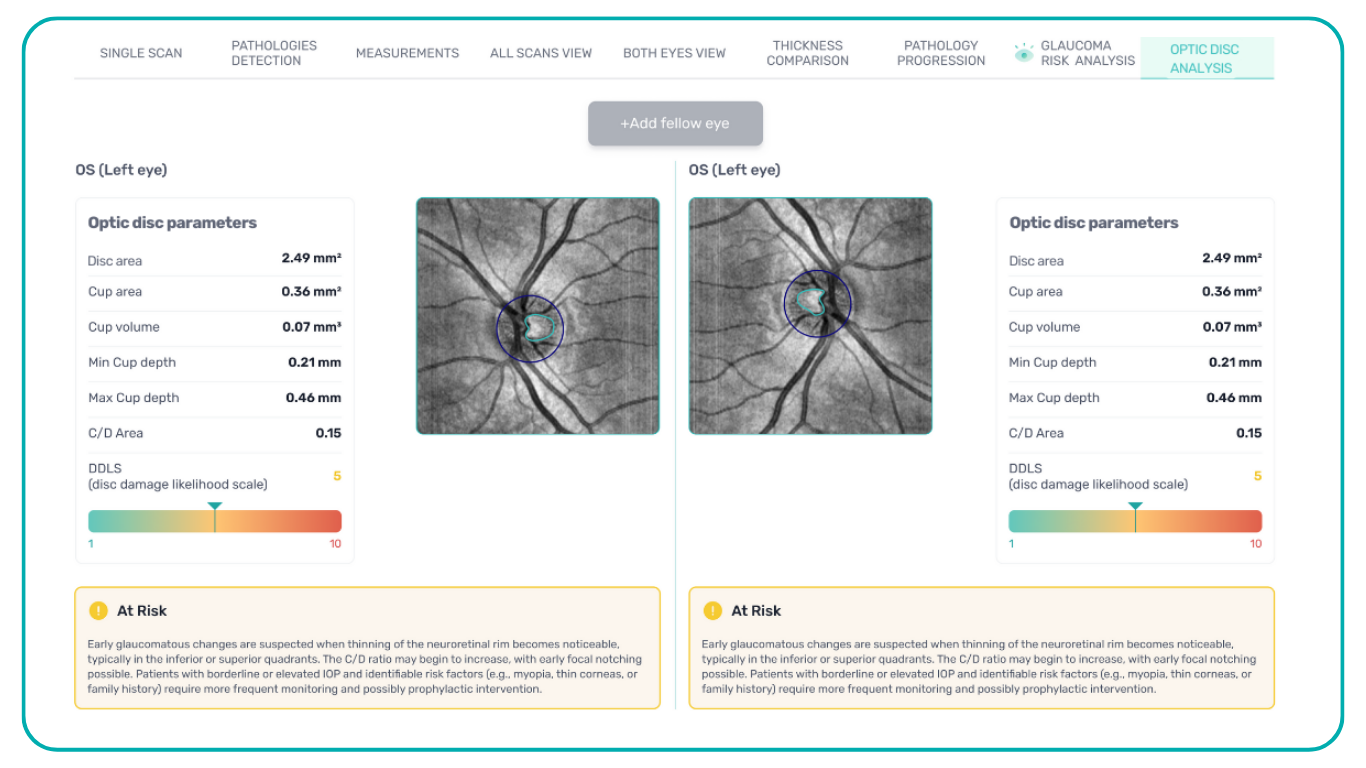
One example of promising AI technology is Altris AI, artificial intelligence for OCT scan analysis, which has introduced its Advanced Optic Disc (OD) Analysis that provides a comprehensive picture of the optic disc’s structural damage, allowing detailed glaucoma assessment for treatment choice and monitoring.

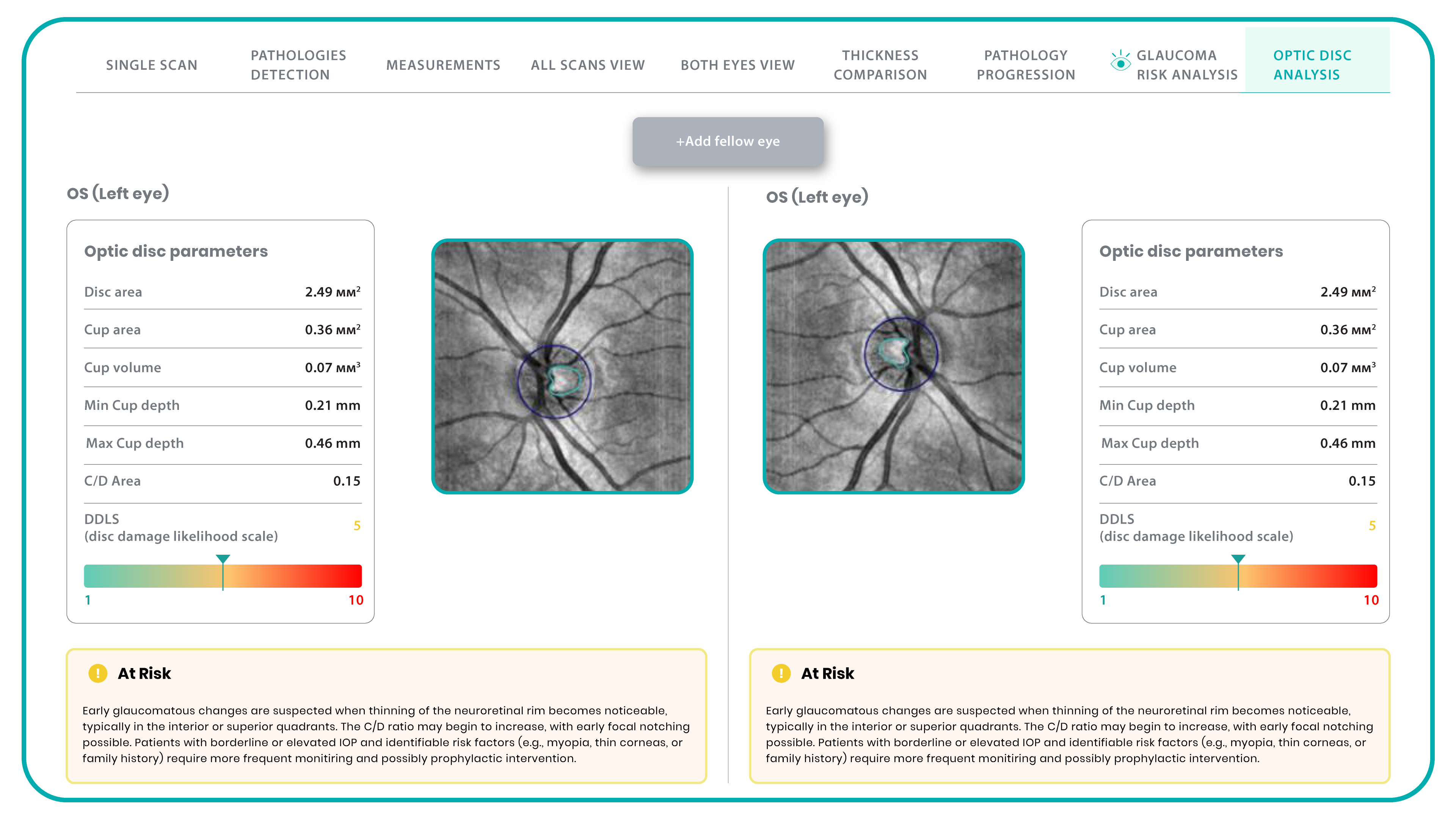
This OD module evaluates optic disc parameters using OCT, providing personalized assessments by accounting for individual disc sizes and angle of rim absence. Such a tailored approach eliminates reliance on normative databases, making evaluations more accurate and patient-specific.
Furthermore, it enables cross-evaluation across different OCT systems, allowing practitioners to analyze macula and optic disc pathology, even when data originates from multiple OCT devices. Key parameters evaluated by Altris AI’s Optic Disc Analysis include disc area, cup area, cup volume, minimal and maximum cup depth, cup/disc area ratio, rim absence angle, and disc damage likelihood scale (DDLS).
AI for Clinical Trials and Research
AI is revolutionizing clinical trials and research in ophthalmology. One such key application of AI is biomarker discovery and analysis. Algorithms can analyze large datasets of medical images, such as OCT scans, to identify and quantify biomarkers for various eye diseases. These biomarkers can be used to assess disease progression, monitor treatment response, and predict clinical outcomes.
AI is also being used to improve the efficiency and effectiveness of clinical trials. By automating the process of identifying eligible patients for clinical trials, AI can help researchers recruit participants more quickly and ensure that trials include appropriate patient populations, accelerating the development of new treatments.
Algorithms can analyze real-world data (RWD) collected from electronic health records and other sources to generate real-world evidence (RWE). RWE provides valuable insights into disease progression, treatment patterns, and long-term outcomes in everyday clinical settings, complementing the findings of traditional randomized controlled trials.
Oculomics
Integrating digitized big data and computational power in multimodal imaging techniques has presented a unique opportunity to characterize macroscopic and microscopic ophthalmic features associated with health and disease, a field known as oculomics. To date, early detection of dementia and prognostic evaluation of cerebrovascular disease based on oculomics has been realized. Exploiting ophthalmic imaging in this way provides insights beyond traditional ocular observations.
For example, the NeurEYE research program, led by the University of Edinburgh, is using AI to analyze millions of anonymized eye scans to identify biomarkers for Alzheimer’s disease and other neurodegenerative conditions. This research can potentially revolutionize early detection and intervention for these devastating diseases.
Another effort spearheaded by researchers from Penn Medicine, Penn Engineering is exploring the use of AI to analyze retinal images for biomarkers indicative of cardiovascular risk. AI systems are being trained on fundus photography to detect crucial indicators, such as elevated HbA1c levels, a hallmark of high blood sugar, and a significant risk factor for both diabetes and cardiovascular diseases.
AI analysis of retinal characteristics, such as retinal thinning, vascularity reduction, corneal nerve fiber damage, and eye movement, has shown promise in predicting Neurodegenerative diseases. Specifically, decreases in retinal vascular fractal dimension and vascular density have been identified as potential biomarkers for early cognitive impairment, while reductions in the retinal arteriole-to-venular ratio correlate with later stages.
Moving from AI, we now turn to another significant trend identified in our survey:
Optogenetics
Optogenetics represents a significant leap forward in ophthalmic therapeutics, offering a potential solution for vision restoration in patients with advanced retinal degenerative diseases, where traditional gene therapy often falls short. While gene replacement therapies are constrained by the need for viable target cells and the complexity of multi-gene disorders like retinitis pigmentosa (RP), optogenetics offers a broader approach.
This technique aims to circumvent the loss of photoreceptors by introducing light-sensitive proteins, known as opsins, into the surviving inner retinal cells and optic nerve, restoring visual function through light modulation. This method is particularly advantageous as it is agnostic to the specific genetic cause of retinal degeneration.
By delivering opsin genes to retinal neurons, the technology enables the precise manipulation of cellular activity, essentially transforming these cells into new light-sensing units. This approach can bypass the damaged photoreceptor layer, transmitting visual signals directly to the brain.
Several companies are pioneering advancements in this field. RhyGaze, for example, has secured substantial funding to accelerate the development of its lead clinical candidate, a novel gene therapy designed for optogenetic vision restoration. Their efforts encompass preclinical testing, including pharmacology and toxicology studies, an observational study to define clinical endpoints, and a first-in-human trial to assess safety and efficacy. The success of RhyGaze’s research could pave the way for widespread clinical applications, significantly impacting the treatment of blindness globally.
Nanoscope Therapeutics is also making significant strides with its MCO-010 therapy. This investigational treatment, administered through a single intravitreal injection, delivers the Multi-Characteristic Opsin (MCO) gene, enabling remaining retinal cells to function as new light-sensing cells. Unlike earlier optogenetic therapies that required bulky external devices, MCO-010 eliminates the need for high-tech goggles, simplifying the treatment process and enhancing patient convenience. The ability to restore light sensitivity without external devices represents a major advancement, potentially broadening the applicability of optogenetics to a wider patient population.
Another critical area of innovation highlighted in our survey is the advancement of treatments for AMD and GA.
New AMD/GA Treatment
Age-related macular degeneration (AMD) and geographic atrophy (GA) represent a significant challenge in ophthalmology, demanding innovative therapeutic strategies beyond the established anti-VEGF paradigm.
Gene Correction
Gene editing is emerging as a powerful tool in the fight against AMD and GA, potentially correcting the underlying genetic errors that contribute to these diseases. Essentially, it allows us to make precise changes to a patient’s DNA.
Traditional gene editing techniques often rely on creating ‘double-strand breaks’ (DSBs) in the DNA at specific target sites, which are like precise cuts in the DNA strand. These cuts are made using specialized enzymes, like CRISPR-Cas9, which act as molecular scissors. While effective, these methods can sometimes introduce unwanted changes at the cut site, such as small insertions or deletions.
After a DSB is made, the cell’s natural repair mechanisms kick in. There are two main pathways:
- Non-Homologous End Joining (NHEJ): This is the cell’s quick-fix method. It essentially glues the broken ends back together. However, this process can sometimes introduce errors, leading to small insertions or deletions that can disrupt the gene’s function.
- Homology-Directed Repair (HDR): This is a more precise repair method. It uses a ‘donor’ DNA template to guide the repair process, ensuring accuracy. However, HDR is more complex and less efficient, especially in non-dividing cells.
To overcome these limitations of traditional gene editing, researchers have developed more precise techniques:
- Base Editing: This technique allows scientists to change a single ‘letter’ in the DNA code without creating DSBs.
- Prime Editing: This advanced technique builds upon CRISPR-Cas9, allowing for a wider range of precise DNA changes. It can correct most disease-causing mutations with enhanced safety and accuracy.
- CASTs (CRISPR-associated transposases): This method enables larger DNA modifications without creating DSBs, offering a safer approach to genetic correction.
Why does this matter for AMD and GA? These advancements in gene editing are crucial for addressing the genetic roots of these pathologies. We can potentially develop more effective and targeted therapies by precisely correcting the faulty genes that contribute to these diseases. The technologies are still being researched, but they hold great promise for the future of ophthalmology.
Cell Reprogramming
Cell reprogramming offers a novel approach to regenerative medicine, with the potential to replace damaged retinal cells. This technique involves changing a cell’s fate, either in vitro or in vivo. In vitro reprogramming involves extracting cells, reprogramming them in a laboratory, and then transplanting them back into the patient. In vivo reprogramming, which directly reprograms cells within the body, holds particular promise for retinal diseases. This approach has succeeded in preclinical studies, demonstrating the potential to restore vision in conditions like congenital blindness.
Vectors and Delivery Methods
The success of gene therapy relies on efficiently delivering therapeutic genes to target retinal cells. Vectors are essentially delivery vehicles, designed to carry therapeutic genes into cells. These vectors can be broadly classified into two categories: viral and non-viral. Vectors, both viral and non-viral, are crucial for this process.
Viral vectors are modified viruses that have been engineered to remove their harmful components and replace them with therapeutic genes. They are highly efficient at delivering genes into cells, as they have evolved to do just that. Adeno-associated viruses (AAVs) are the most commonly used viral vectors in ocular gene therapy due to their safety profile and cell-specificity. The diversity of AAV serotypes allows for tailored gene delivery to specific retinal cell types.
Non-viral vectors, on the other hand, are synthetic systems that don’t rely on viruses. They can be made from lipids, polymers, or even DNA itself. While they may be less efficient than viral vectors, they offer safety and ease of production advantages.
Advances in vector design, whether viral or non-viral, are focused on enhancing gene expression, cell-specificity, and carrying capacity.
Now, let’s examine the ongoing evolution of anti-VEGF treatments, a cornerstone of modern retinal care.
New Anti-VEGF drugs
The landscape of ophthalmology has undergone a dramatic transformation since the early 1970s when Judah Folkman first proposed the concept of tumor angiogenesis. His idea sparked research that ultimately led to the identification of vascular endothelial growth factor (VEGF) in 1989 and the development of anti-VEGF therapies, revolutionizing the treatment of neovascular eye diseases, dramatically improving outcomes for patients with wet AMD, diabetic retinopathy, and retinal vein occlusions.
Population-based studies have shown a substantial reduction (up to 47%) in blindness due to wet AMD since the introduction of anti-VEGF therapies. However, significant gaps remain despite this progress, especially regarding treatment durability. Anti-VEGF drugs require frequent intravitreal injections, which can be difficult for patients due to time commitments, financial costs, and potential discomfort. Although newer agents have extended treatment intervals, patient adherence and undertreatment challenges persist in real-world settings. Innovative approaches are being investigated to address these unmet needs to increase drug durability and reduce the treatment burden.
Tyrosine Kinase Inhibitors
One approach to increasing treatment durability is using tyrosine kinase inhibitors (TKIs). TKIs are small-molecule drugs that act as pan-VEGF blockers by binding directly to VEGF receptor sites inside cells, offering a different action mechanism than traditional anti-VEGF drugs that target circulating VEGF proteins.
Currently, TKIs are being investigated as maintenance therapy, primarily in conjunction with sustained-release delivery systems. Two promising TKIs for retinal diseases are axitinib and vorolanib. In a bioresorbable hydrogel implant, Axitinib is being studied for neovascular AMD and diabetic retinopathy. Vorolanib, in a sustained-release delivery system, is also being investigated for neovascular AMD. These TKIs offer the potential for less frequent dosing, reducing the treatment burden for patients.
Port Delivery System
The Port Delivery System (PDS) is a surgically implanted, refillable device that provides continuous ranibizumab delivery for up to 6 months. While it’s FDA-approved for neovascular AMD, it’s also being investigated for other retinal diseases, such as diabetic macular edema and diabetic retinopathy.
Although the PDS faced a voluntary recall due to issues with septum dislodgment, it has returned to the market with modifications. The PDS offers the potential for significantly reduced treatment frequency for a subset of patients. However, challenges remain, including the need for meticulous surgical implantation and the risk of endophthalmitis.
Nanotechnology
Nanotechnology offers promising solutions to overcome limitations of current ocular drug delivery. The unique structure of the eye, with its various barriers, poses challenges for drug delivery. Topical administration often fails to achieve therapeutic concentrations, while frequent intravitreal injections carry risks. Nanotechnology can improve drug solubility, permeation, and bioavailability through nanoparticles, potentially extending drug residence time and reducing the need for frequent injections. Several nanoparticle systems, lipid and polymeric, are being studied for ocular drug delivery, offering hope for more effective and less invasive treatments.
FDA-cleared AI for OCT analysis
Summing up
The advancements discussed in this article, encompassing AI, optogenetics, novel AMD/GA therapies, and refined anti-VEGF treatments, collectively signal a transformative era for ophthalmology. As highlighted by the survey results, AI probably encompasses most of the changes by redefining diagnostic and clinical workflows through its capacity for image analysis, biomarker identification, and personalized patient management.
Optogenetics offers a distinct pathway to vision restoration, bypassing limitations of traditional gene therapy. The progress in AMD/GA treatments, particularly gene editing and cell reprogramming, presents opportunities for targeted interventions. Finally, the evolution of anti-VEGF therapies, with innovations in drug delivery and sustained-release mechanisms, addresses persistent challenges in managing neovascular diseases.
These developments, driven by technological innovation and clinical research, promise to enhance patient outcomes and reshape the future of ophthalmic care.
-
Altris AI Launches Advanced Optic Disc Analysis for Glaucoma, Complementing GCC Asymmetry Analysis
 Maria Znamenska
1 min.
Maria Znamenska
1 min.Altris AI, a leading force in AI for OCT scan analysis that detects the widest range of retina pathologies and biomarkers, launches an advanced glaucoma Optic Disc Analysis module.
Early detection of glaucoma demands exceptional precision, as the early signs are often subtle and difficult to detect. A major challenge in glaucoma screening is the high rate of false positive referrals, which can lead to unnecessary appointments in secondary care. This not only burdens healthcare systems but also causes anxiety for patients. Yet delayed or missed detection of glaucoma results in irreversible vision loss for millions of people worldwide. So the need for timely and accurate glaucoma detection has never been so critical in the eye care industry, and automated AI-powered glaucoma analysis will offer a transformative potential to improve outcomes.
To address this critical need, Altris AI has introduced its Advanced Optic Disc (OD) Analysis, building on its earlier innovation with Ganglion Cell Complex (GCC) Asymmetry Analysis to enhance the improvements from the Altris AI macula module which has been available for several years.
Altris AI’s glaucoma detection journey began with the creation of AI-powered GCC Asymmetry Analysis, designed to detect early risk of glaucoma.
In February 2025 Altris launched the AI-powered Advanced Optic Disc (OD) Analysis module as OD analysis is regarded as the gold standard for structural glaucoma diagnosis.
This method provides a comprehensive picture of structural damage and allows detailed glaucoma assessment for treatment choice and monitoring.
The module evaluates optic disc parameters using OCT, providing personalized assessments by accounting for individual disc sizes and angle of rim absence. This tailored approach eliminates reliance on normative databases, making evaluations more accurate and patient-specific.
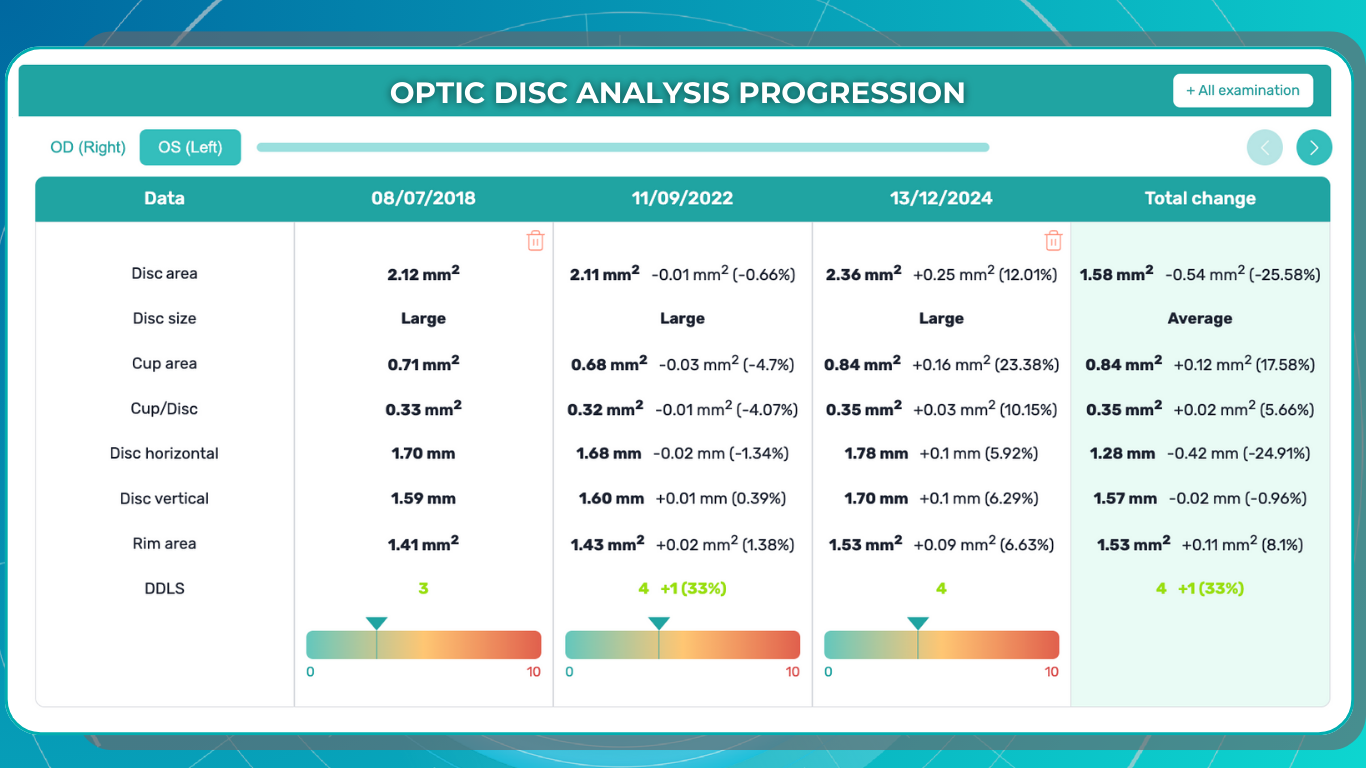
Altris AI’s platform assigns a severity score for optic disc damage on a scale from 1 to 10, offering valuable insights into glaucomatous changes. Furthermore, it enables cross-evaluation across different OCT systems, allowing practitioners to analyze both macula and optic disc pathology, even when data originates from multiple OCT devices.
Optic Disc Analysis for Glaucoma: Key Parameters
- Disc area
- Cup area
- Cup volume
- Minimal Cup depth
- Maximum Cup depth
- Cup/Disc area ratio
- Rim Absence angle
- Disc-Damage Likelihood Scale (DDLS)
The Altris AI Glaucoma Module is compatible with various OCT scan protocols, including:
- 3D OCT optic disc scans
- 3D OCT horizontal wide scans
- 3D OCT vertical-wide scans
- OCT optic disc raster scans
By combining GCC Asymmetry and Advanced Optic Disc analysis for glaucoma empower enabling Eyecare practitioners (ECPs) to make faster evaluations and explore a wider range of treatment options. This streamlined approach empowers ECPswith timely, actionable data, ultimately improving patient outcomes and care.
Dr. Maria Znamenska, MD, PhD, and a Chief Medical Officer at Altris AI, commented:
“The launch of our Advanced Optic Disc Analysis module marks a pivotal step forward in glaucoma care. By combining the gold standard of optic disc evaluation with AI-powered precision, we’re equipping eye care professionals with the tools to make more accurate and timely diagnosis of this vision-threatening disorder. This innovation not only reduces false positive referrals but also enhances early detection and treatment planning—ensuring better outcomes for patients and optimizing healthcare resources. Together with GCC asymmetry analysis, our platform empowers clinicians to elevate the standard of glaucoma care, offering hope to millions at risk of vision loss.”
About Altris AI
Altris AI is an artificial intelligence platform for OCT analysis, capable of detecting the widest range of retinal pathologies and biomarkers on the market – more than 70. Leading the way in AI innovation, Altris AI provides transformative solutions that enhance the diagnosis, treatment, and monitoring of retinal diseases, enabling eye care professionals to deliver exceptional patient care.
-
ML Applied to 3D Optic Disc Analysis for Glaucoma Risk Assessment Across Different OCT Scan Protocols Without a Normative Database
Angelina Hramatik
14.02.202520 min readMachine Learning Applied to 3D Optic Disc Analysis for Glaucoma Risk Assessment Across Different OCT Scan Protocols Without a Normative Database
1. Introduction
Glaucoma is one of the leading causes of irreversible blindness worldwide, affecting millions of people annually. The disease is often asymptomatic in its early stages, making timely diagnosis particularly challenging. Early detection of glaucomatous changes is crucial for preventing vision loss and improving long-term patient outcomes.
One well-established method for assessing glaucoma is the Disc Damage Likelihood Scale (DDLS), which evaluates structural changes in the optic nerve head (ONH) based on the extent of neuroretinal rim loss. This method categorizes glaucomatous damage severity by analyzing the relationship between the optic cup and neural rim, while also accounting for optic disc size without relying on a normative database. 1, 2, 3, 4.
While DDLS is recognized for its reliability and utility in clinical practice, it is not a standalone diagnostic tool. Rather, it is one of several methods used to identify signs of glaucoma, and its implementation is often limited to specific imaging modalities or scan protocols, such as 3D optic disc-only scans or fundus images.
In this article, we introduce an enhanced approach to DDLS analysis that overcomes these limitations. We want to present a solution, which is capable of performing DDLS analysis on any OCT scan protocol that captures the optic nerve, including 3D optic disc scans (which provide the most detailed view of the nerve), as well as OCT horizontal and vertical 3D wide scans. By leveraging advanced machine learning models, we achieve unprecedented flexibility and accuracy, ensuring reliable analysis across different scanning protocols and OCT systems.
Unlike traditional systems restricted to specific devices or data formats, our solution processes scans from multiple OCT systems. Moreover, it excels in challenging scenarios, providing clinicians with a robust and versatile tool for analyzing potential signs of glaucoma.
FDA-cleared AI for OCT analysis
A Brief Theoretical Overview
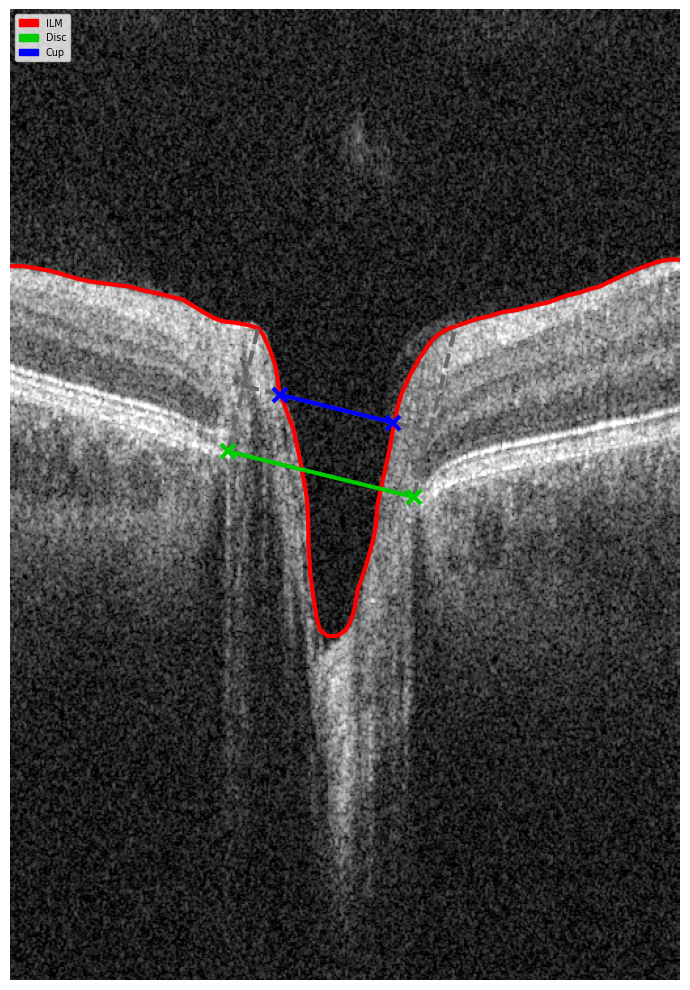
Optical coherence tomography (OCT) scans vary in the anatomical regions they capture. One specific type is the optic disc OCT scan (Figure 2), which provides high-resolution imaging of the optic disc and the surrounding optic nerve head (ONH) structures. This scan type is commonly used in glaucoma assessment, as it allows for the evaluation of the optic nerve’s structure, including the neuroretinal rim, optic cup, and surrounding peripapillary retinal nerve fiber layer (RNFL) — key areas affected in glaucomatous damage.

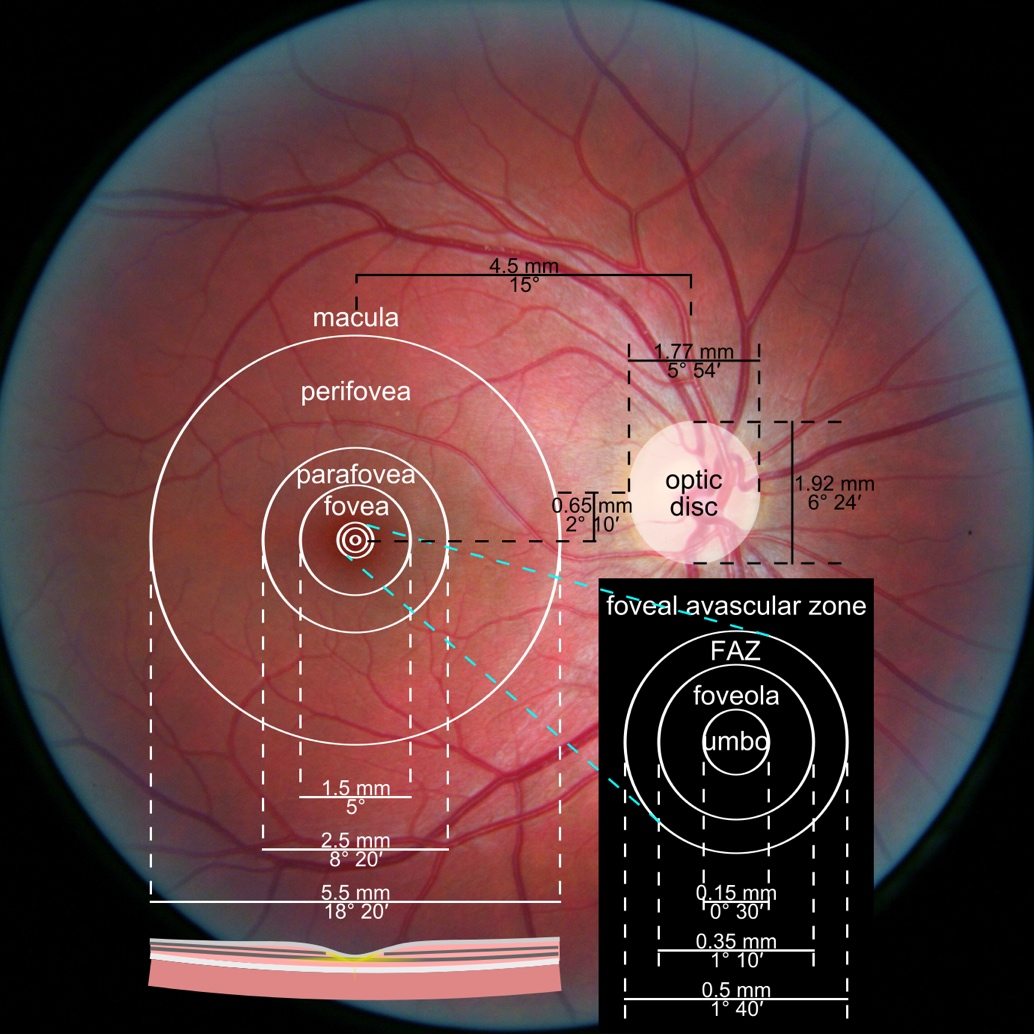
Figure 1. Photograph of the retina of the human eye, with overlay diagrams showing the positions and sizes of the macula, fovea, and optic disc (Reference).

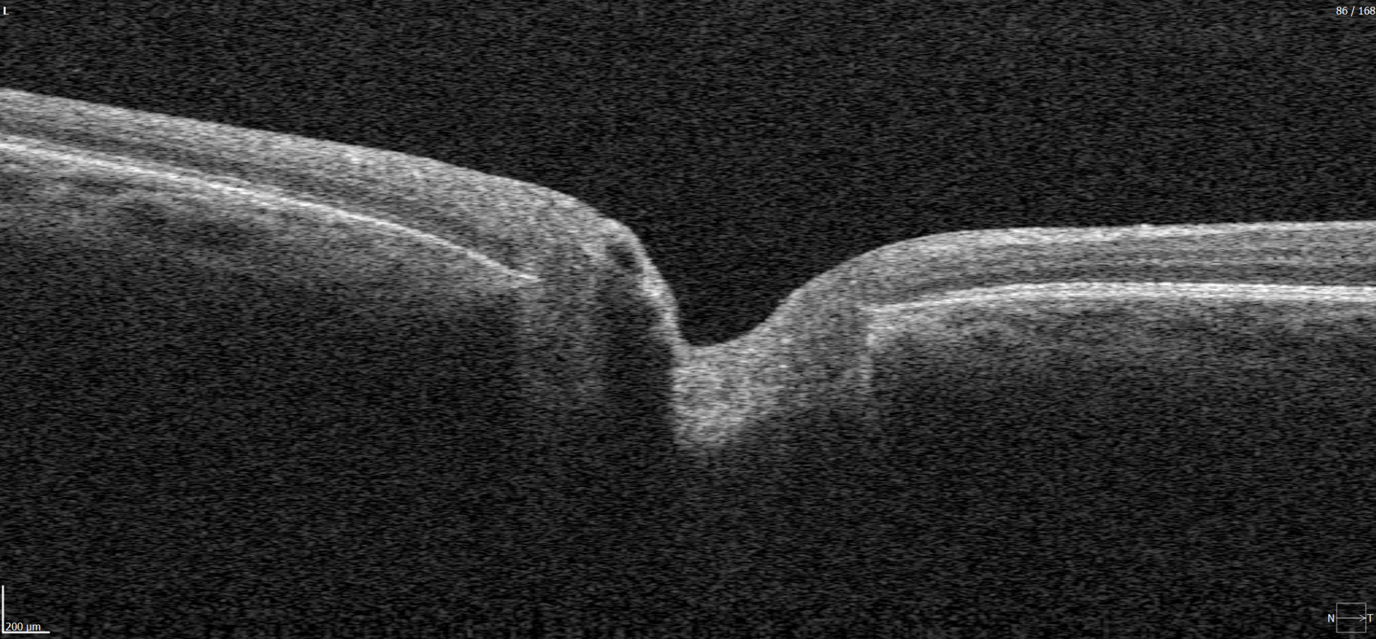
Figure 2. 6 mm OCT b-scan of the optic nerve head (ONH) region.
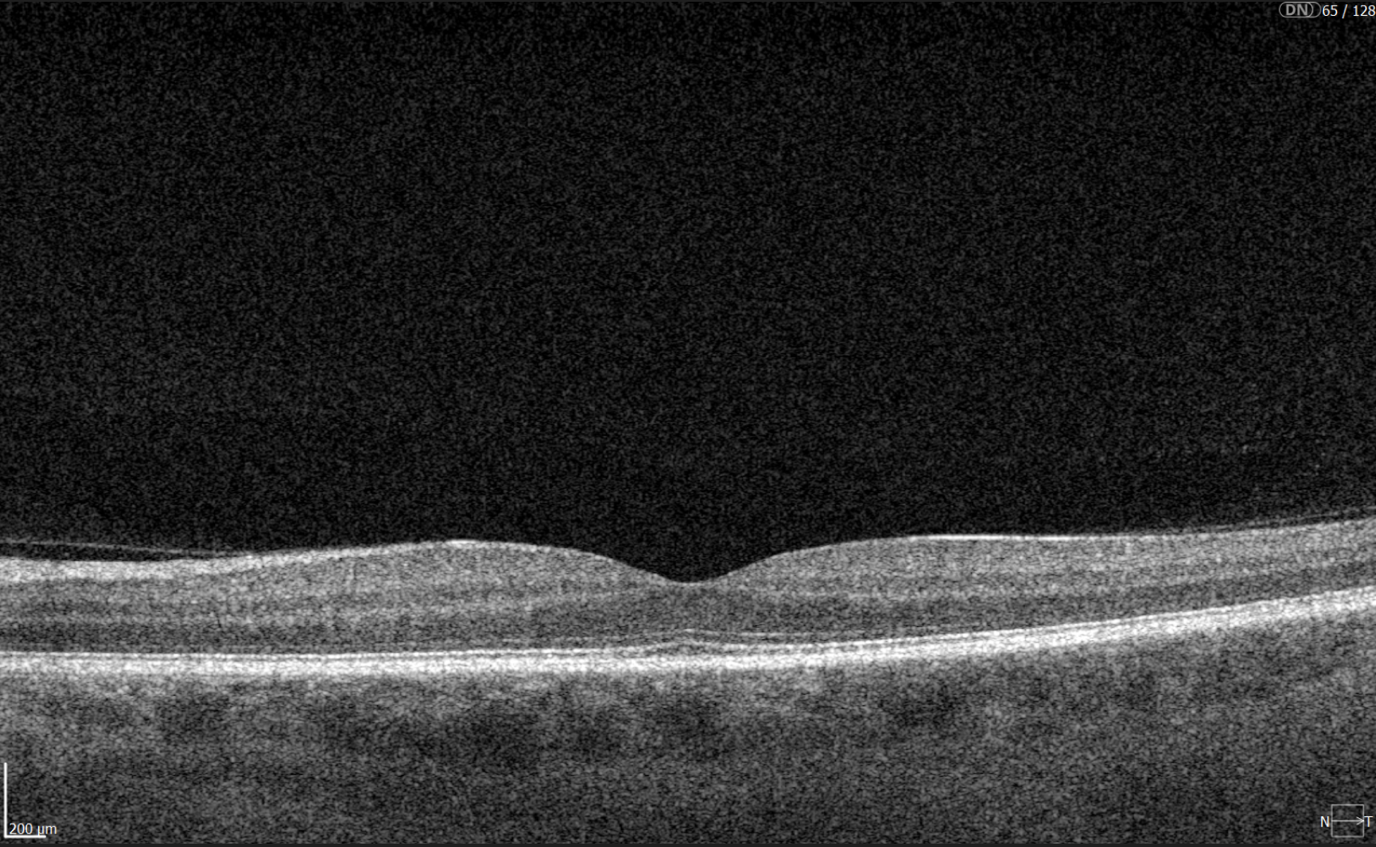
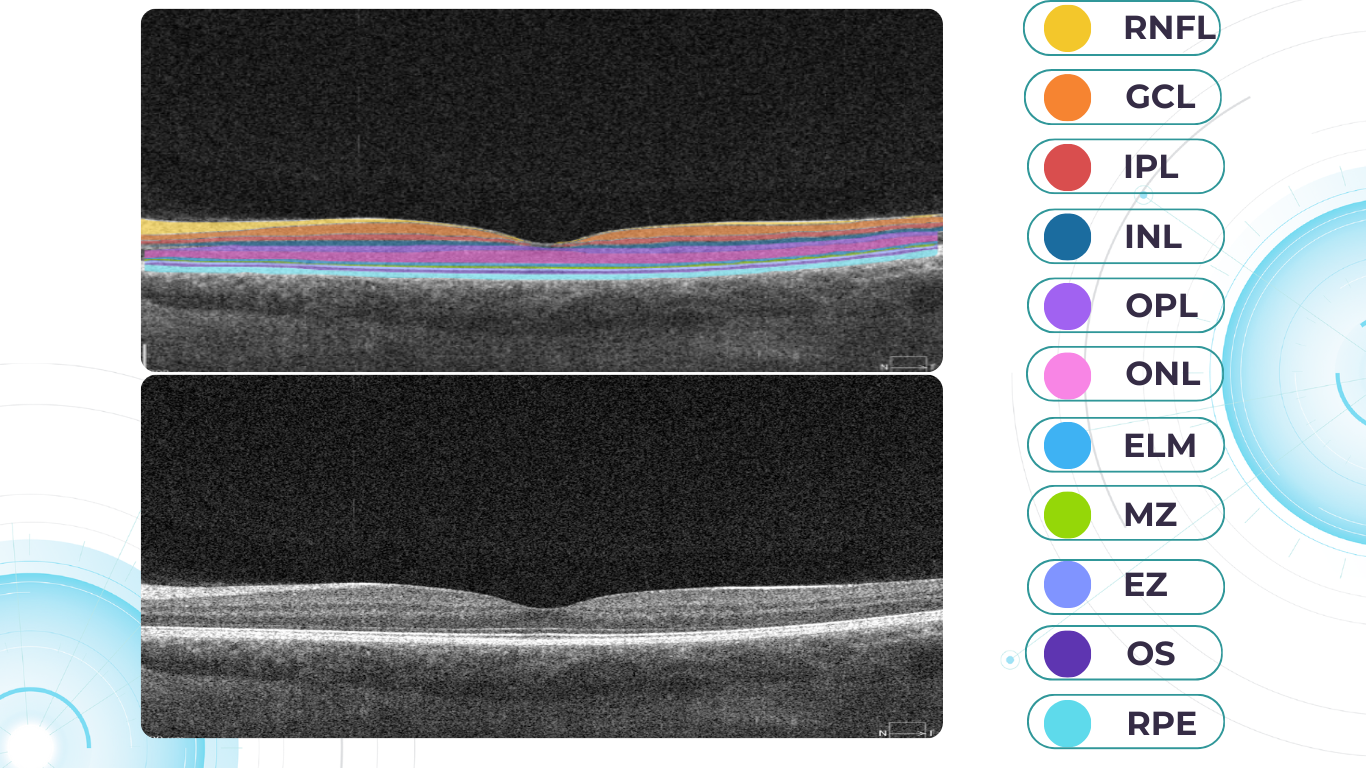
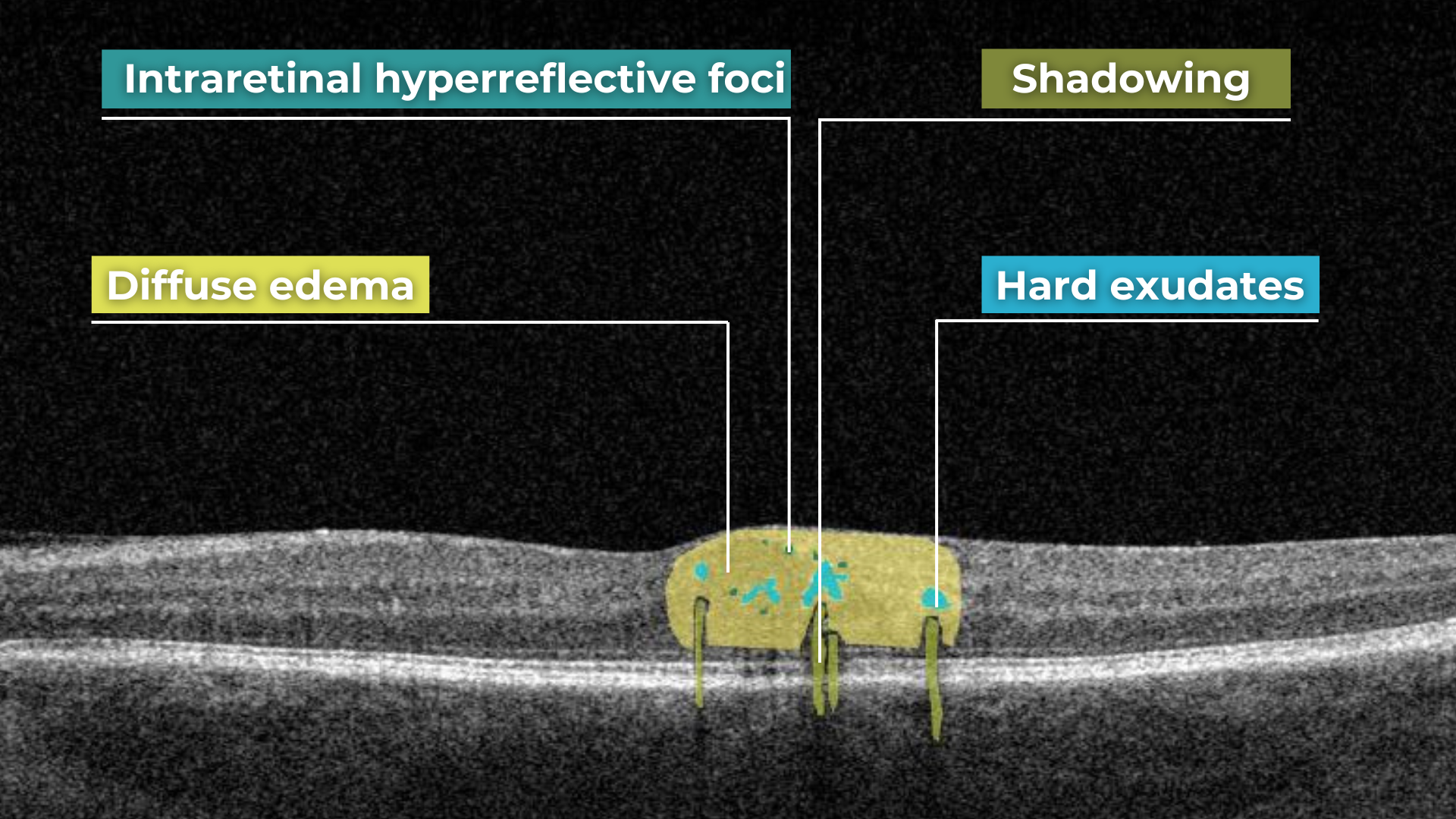
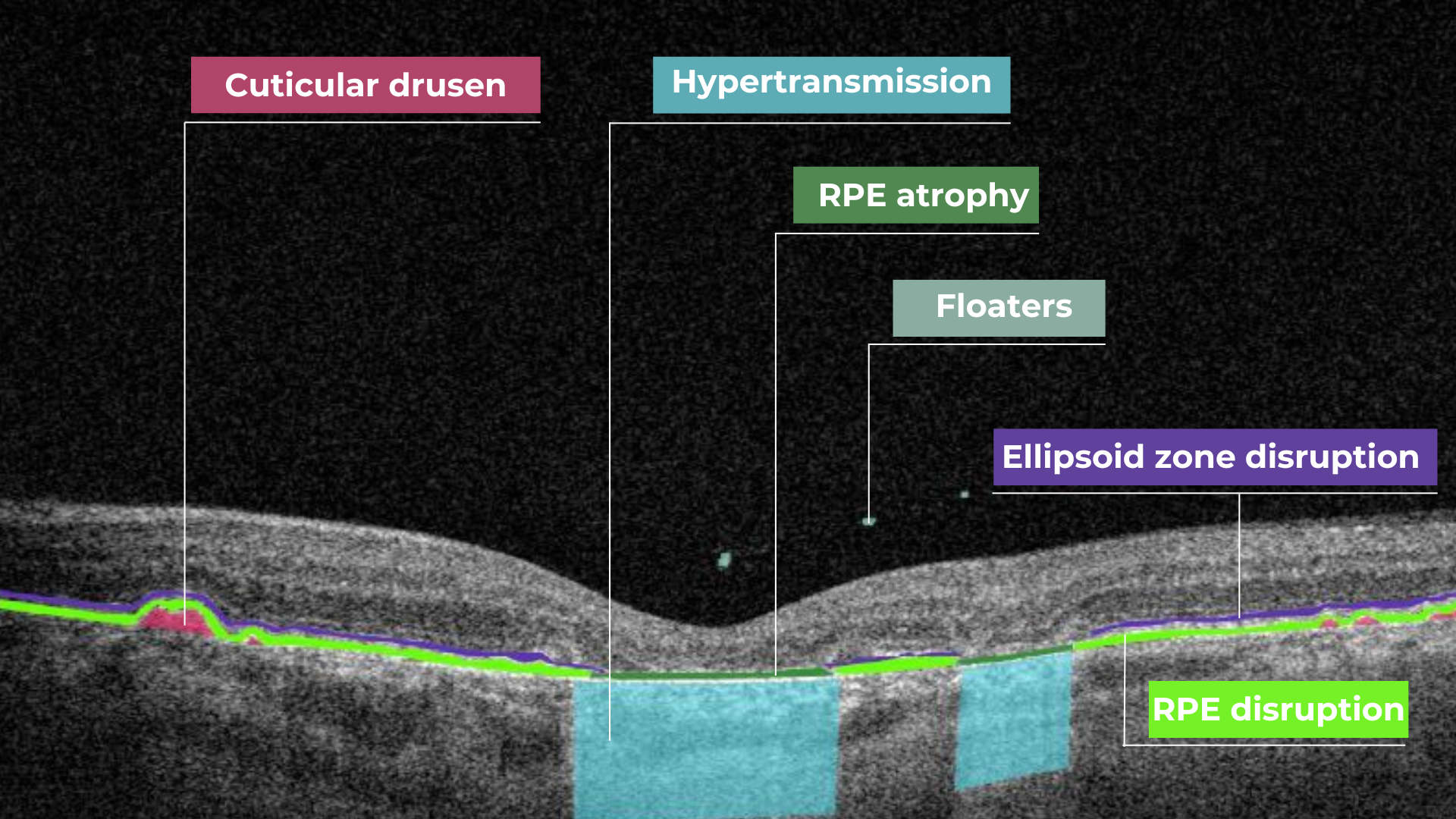
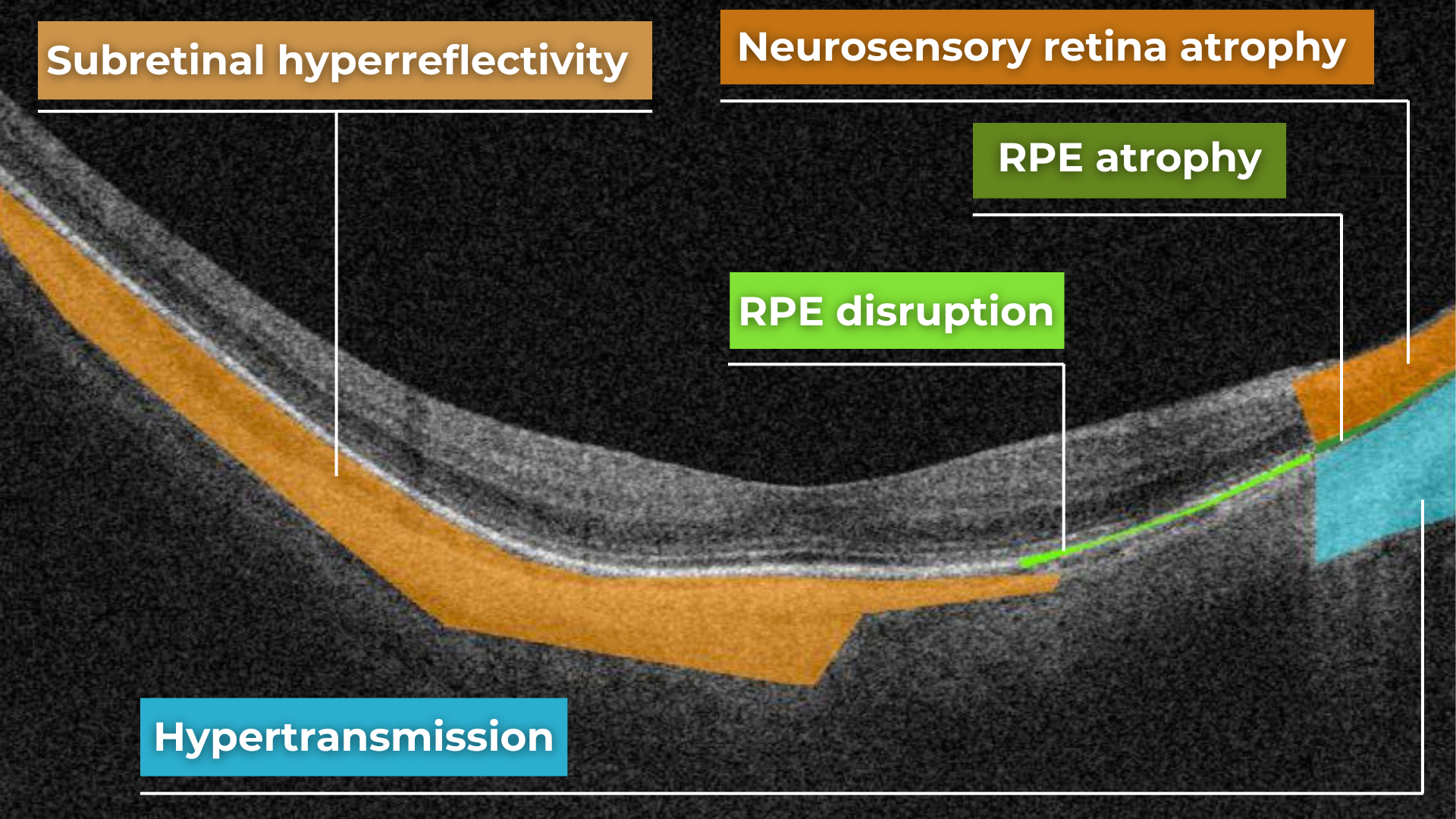
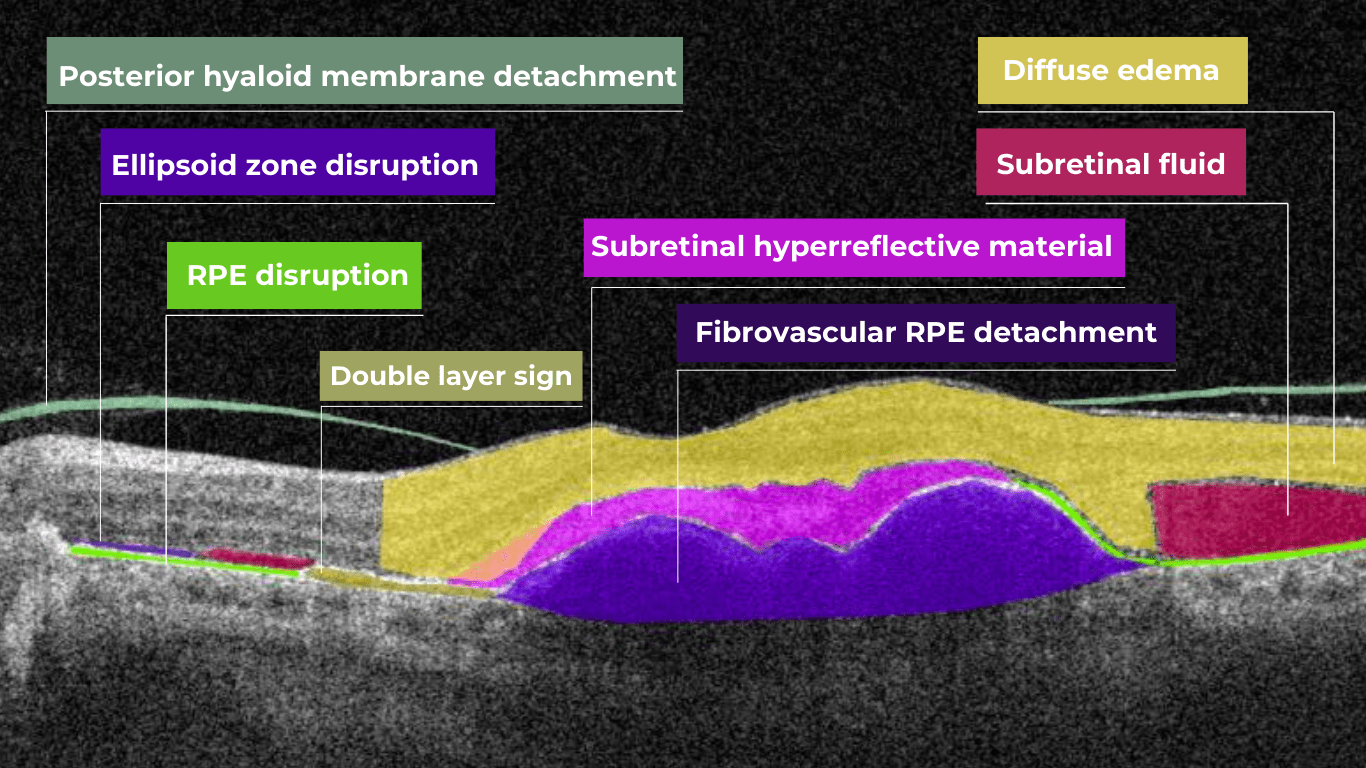
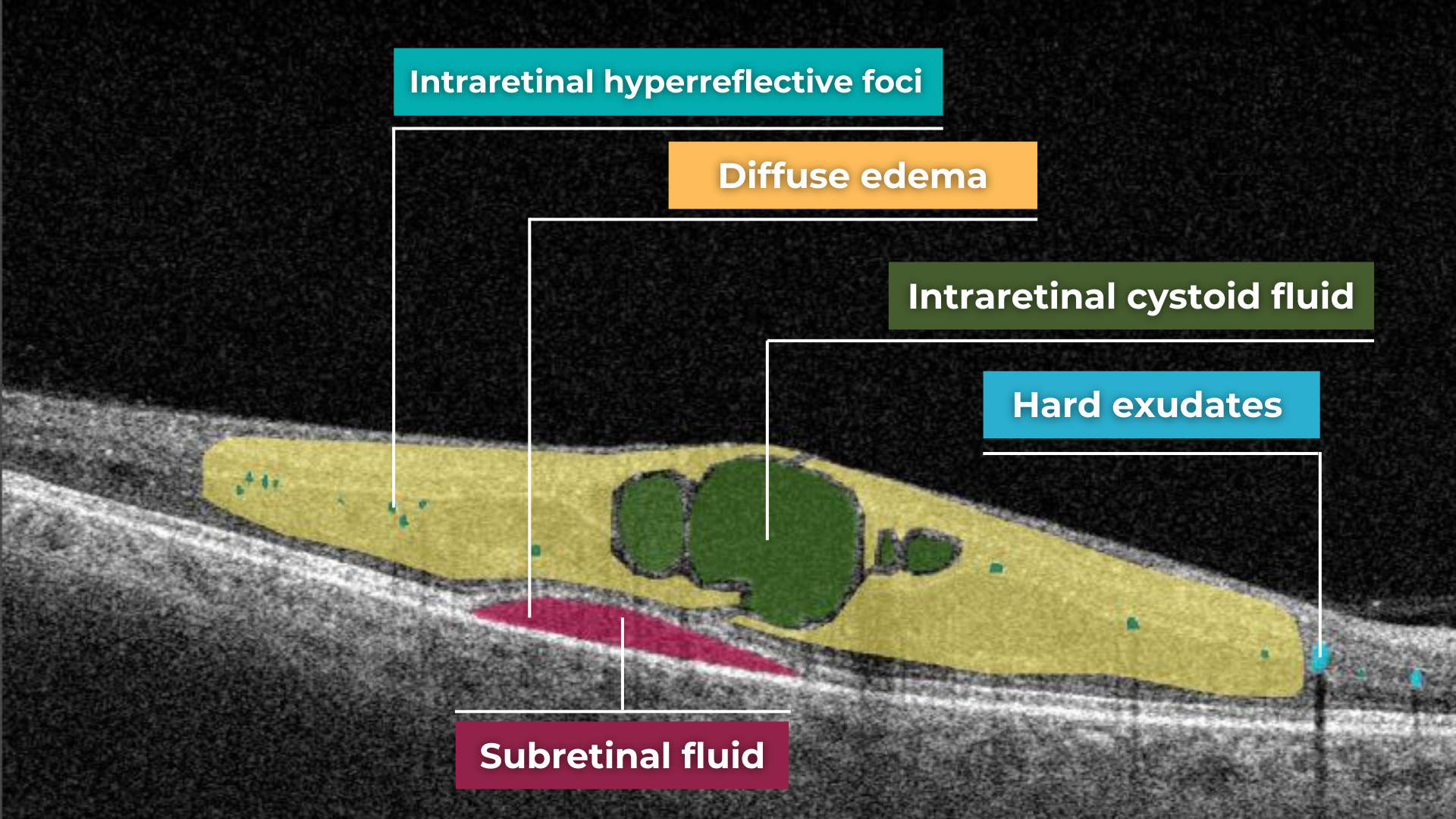
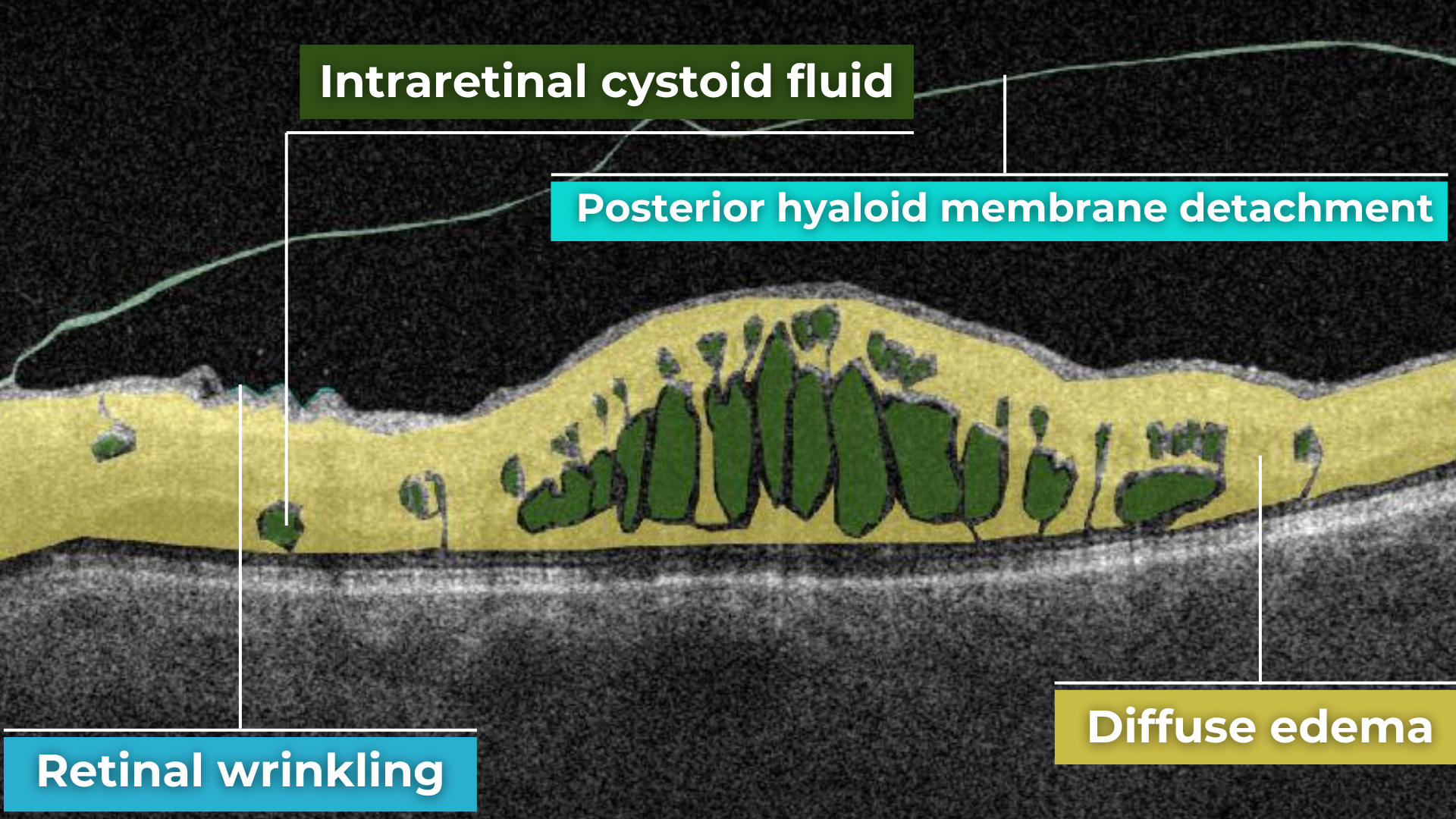
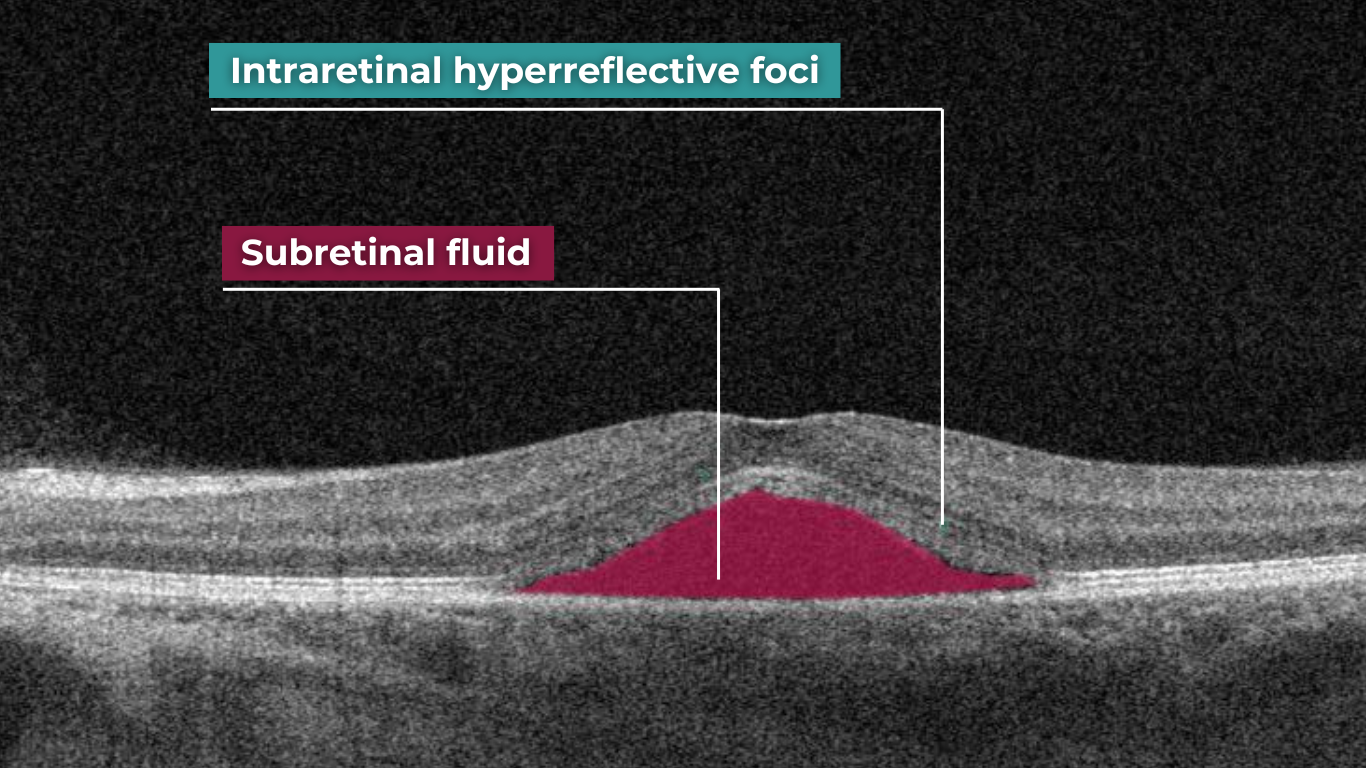
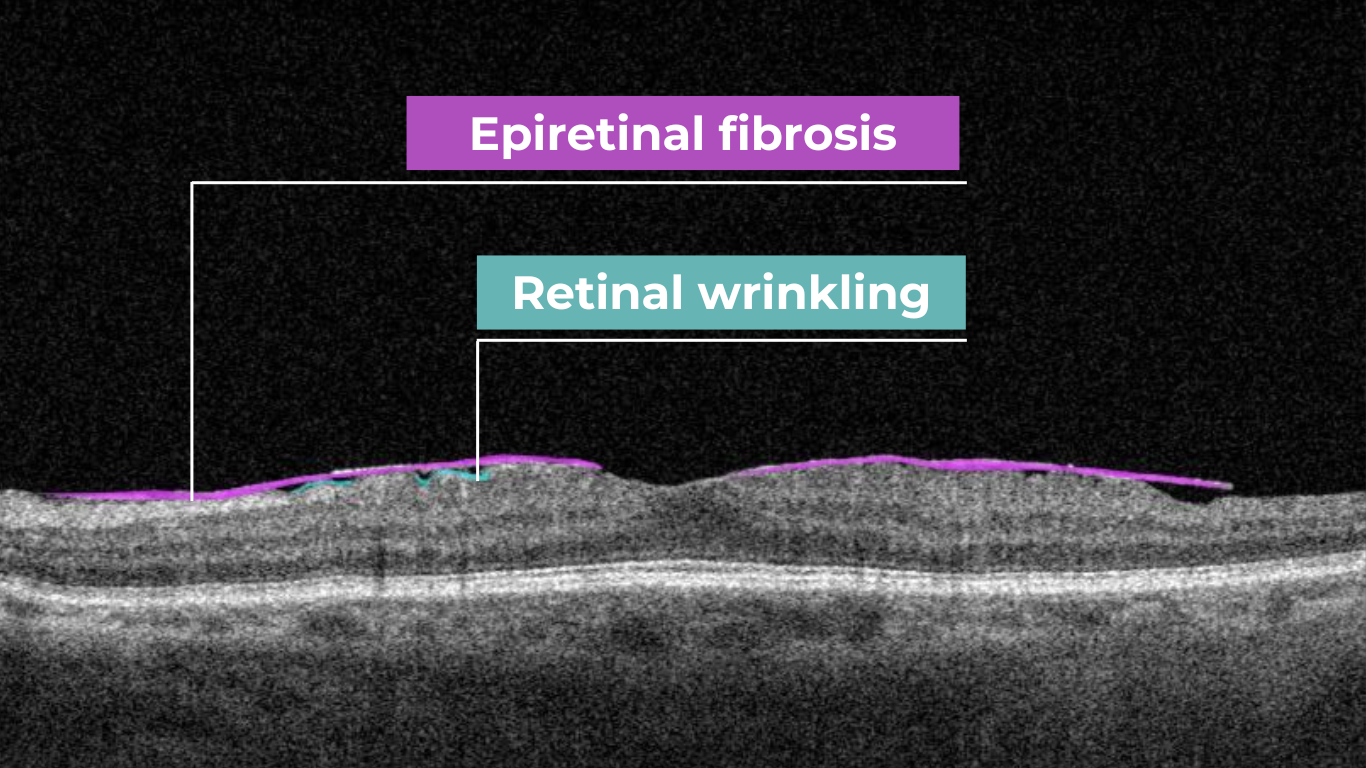
In contrast, macular OCT scans (Figure 3) focus on the central retina, providing detailed visualization of structures such as the foveal center, retinal layers, and macular biomarkers (such as drusen, hypertransmission, fluids etc). Since the macula is anatomically distinct from the optic nerve head, standard macular scans do not capture the ONH comprehensively.

Figure 3. 6 mm OCT b-scan of the macular region, showing the foveal pit and retinal layers.
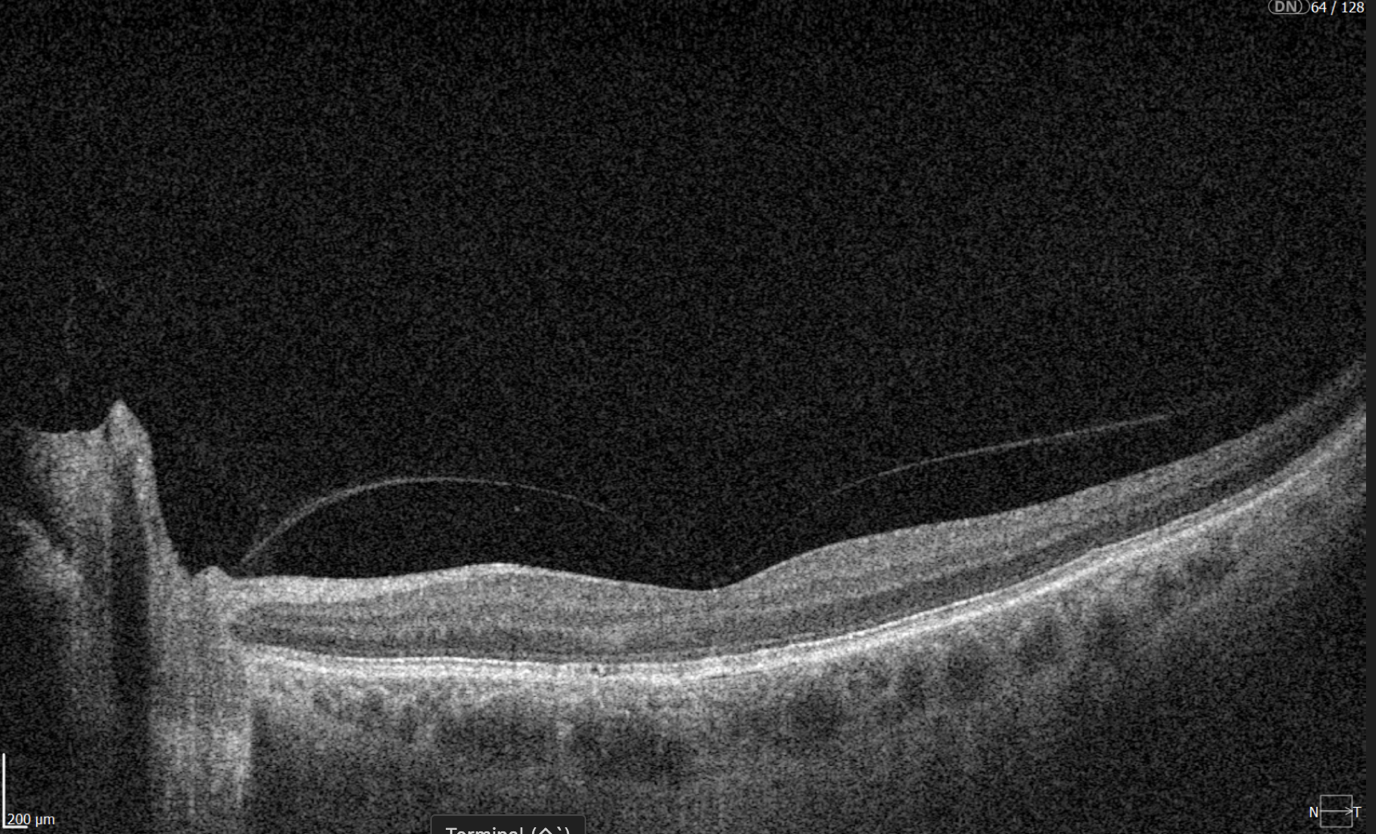
A more comprehensive scanning approach is 12 mm wide scan OCT (Figure 4), which captures both the macular region and optic nerve head in a single scan. This broader field of view allows for the simultaneous assessment of central retinal structures and optic nerve-related changes, making it valuable for detecting and monitoring conditions that affect both regions, such as glaucoma and other neurodegenerative or vascular retinal diseases.

Figure 4. 12 mm wide scan OCT b-scan, which captures both the macular region and part of the optic nerve head.
2. Results
2.1. Experiment Setup
Brief Method Overview
To evaluate the effectiveness of DDLS analysis in assessing glaucoma severity, we designed an experiment comparing results obtained from processing 3D Optic Disc OCT scans and 3D Wide scan OCT scans with the corresponding reports generated by the OCT system. Our method follows four key steps:
- Detecting optic nerve landmarks like Bruch’s Membrane Opening (BMO) points (Eye Keypoints Retrieval / OCT Keypoint Detector Model);
- Segmenting the inner limiting membrane (ILM) (Retina Layers Segmentation Model);
- Reconstructing the neuroretinal rim geometry;
- Applying the Disc Damage Likelihood Scale (DDLS) for classification.
The dataset below was used to validate the algorithm.
Dataset Used for Validating the Entire Algorithm
For validation, we compared our algorithm’s DDLS measurements with the DDLS values generated by the built-in algorithms of the Optopol REVO NX 130 OCT system. This provided a baseline for assessing accuracy and consistency.
To validate our approach, we conducted an experiment comparing DDLS metrics derived from:
- 3D Optic Disc OCT scans, which are traditionally used for DDLS analysis.
- 3D Wide scans, which capture both the macular and optic nerve regions, providing a more comprehensive dataset for analysis.
The dataset includes imaging data from 37 patients examined using the Optopol REVO NX 130 OCT system, with each patient undergoing the following protocols on the same day:
- 3D Optic Disc OCT (6mm zone): 168 scans
- 3D Wide scan (horizontal protocol, 12mm): 128 scans
A report was obtained from the 3D Optic Disc OCT scans, containing all parameters calculated by the device.
Since no manual annotations are available for these data, our comparison is conducted directly against the device-generated results.
The distribution of data was as follows:
- Glaucomatous Optic Disc: 21 cases;
- Normal Optic Disc: 16 cases.
2.2. Final Validation Results: DDLS Accuracy and Error Metrics
To evaluate the performance of our DDLS analysis method, we compared its results with the corresponding DDLS values generated by the OCT device’s built-in algorithms. The device reports serve as a reference point for all calculations, meaning the accuracy, MAE/STD values presented below indicate the level of agreement between our method and the device’s measurements.
The parameters compared below are the key indicators for glaucoma stage assessment.
- The rim-to-disc ratio (RDR) represents the thinnest neuroretinal rim width relative to the vertical optic disc diameter. A lower RDR indicates a more advanced stage of rim thinning, as glaucoma leads to progressive narrowing of the neuroretinal rim due to the loss of ganglion cells axons.
- The rim absence angle (RAA) quantifies the extent of neuroretinal rim loss in degrees. It defines the angle where the rim is completely absent, exposing the optic cup. A wider RAA suggests a more severe stage of glaucoma, as it indicates greater rim loss across the disc circumference.
Both RDR and RAA provide complementary perspectives on structural optic nerve damage:
- RDR measures the smallest remaining rim thickness in proportion to the disc.
- RAA evaluates how much of the disc circumference has lost its rim.
By considering both parameters together, a more comprehensive assessment of glaucoma severity can be achieved. Based on RDR and RAA, a DDLS stage is assigned, allowing for standardized classification of glaucoma progression.

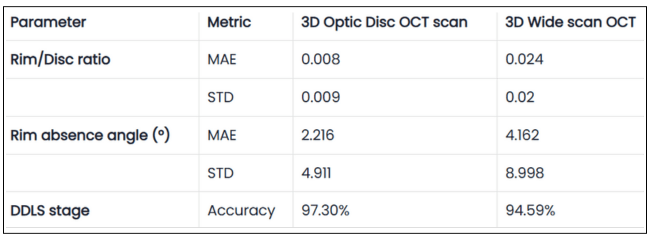
Table 1. Validation Results of DDLS Analysis on 3D Optic Disc and 3D Wide Scan OCT Scans
The table presents validation results comparing 3D Optic Disc OCT scan and 3D Wide scan OCT in DDLS analysis, focusing on Mean Absolute Error (MAE) and Standard Deviation (STD) for key parameters, along with overall DDLS staging accuracy. These metrics are calculated for the rim-to-disc ratio and rim absence angle by comparing their respective values from 3D Optic Disc OCT scans and 3D Wide scans against those from the device reports, providing a precise assessment of deviations from the reference values.
Key Observations
1. Our Goal: Consistency with Device Reports, Not Outperformance
The experiment does not aim to surpass the device’s accuracy but rather to demonstrate that our method produces results in alignment with the device-generated DDLS reports.
The device report serves as a reference, helping to interpret the figures we present, but this does not mean the device’s output is always the absolute truth.
2. High DDLS Staging Accuracy for Both Scan Types
3D Optic Disc OCT scan: 97.3% accuracy in determining DDLS glaucoma stage.
3D Wide scan OCT: 94.59% accuracy, demonstrating strong reliability despite a broader scan area and fewer scans capturing the nerve, leading to less available information.
Conclusion:
- Both types of scans allow the production of clinically reliable DDLS results, but as expected, 3D optic disc scans provide slightly better accuracy due to their higher resolution of the optic nerve head (ONH).
- The small accuracy gap and close values for key parameters between the two suggests that 3D wide scan OCT can still be a viable option for glaucoma assessment, despite offering less detailed information about the optic nerve compared to optic disc scans.
3. RD Ratio and Rim Absence Angle: High Precision Within Clinical Margins
RD Ratio (rim-to-disc ratio):
- Step size between DDLS stages: 0.1.
- Mean Absolute Error (3D Optic Disc OCT scan): 0.008 (significantly smaller than step size).
- Mean Absolute Error (3D Wide scan OCT): 0.024 (still relatively small).
Conclusion:
- Both 3D Optic Disc OCT scan and 3D Wide scan analysis provide high precision in RD ratio calculations.
- The small error ensures that stage classification remains reliable, especially in optic disc scans.
Rim Absence Angle:
- Step size between DDLS stages: Minimum 45°.
- Mean Absolute Error (3D Optic Disc OCT scan): 2.2° (very small compared to step size). Mean Absolute Error (3D Wide scan OCT): 4.2° (still well below stage transition threshold).
Conclusion:
- The method’s margin of error is far smaller than the clinical threshold for stage differentiation, confirming high accuracy in rim loss assessment.
- 3D Optic Disc scans again show better precision, reinforcing that they remain the preferred scan type for DDLS.
4. Our Advantage: Ability to Perform DDLS on Both Scan Types
- Unlike traditional DDLS implementations, which work only with 3D Optic Disc scans, our method can perform DDLS analysis on both 3D Wide scan and 3D Optic Disc OCTs.
- However, 3D Optic Disc OCT remains the preferred method for maximum precision, as it provides a higher-resolution view of the optic nerve.
Key Conclusions
- Our method is unique in its ability to process multiple scan types, while still maintaining high accuracy in both cases.
- On 3D Optic Disc scans, we achieve maximum precision, while on 3D Wide scans, we still maintain clinically reliable accuracy.
- Consistency: Across all glaucoma stages, our method produced stable results that closely matched ground truths provided by medical experts.
- Universal Compatibility: The algorithm performed equally well with scans from other manufacturers, demonstrating its versatility and robustness.
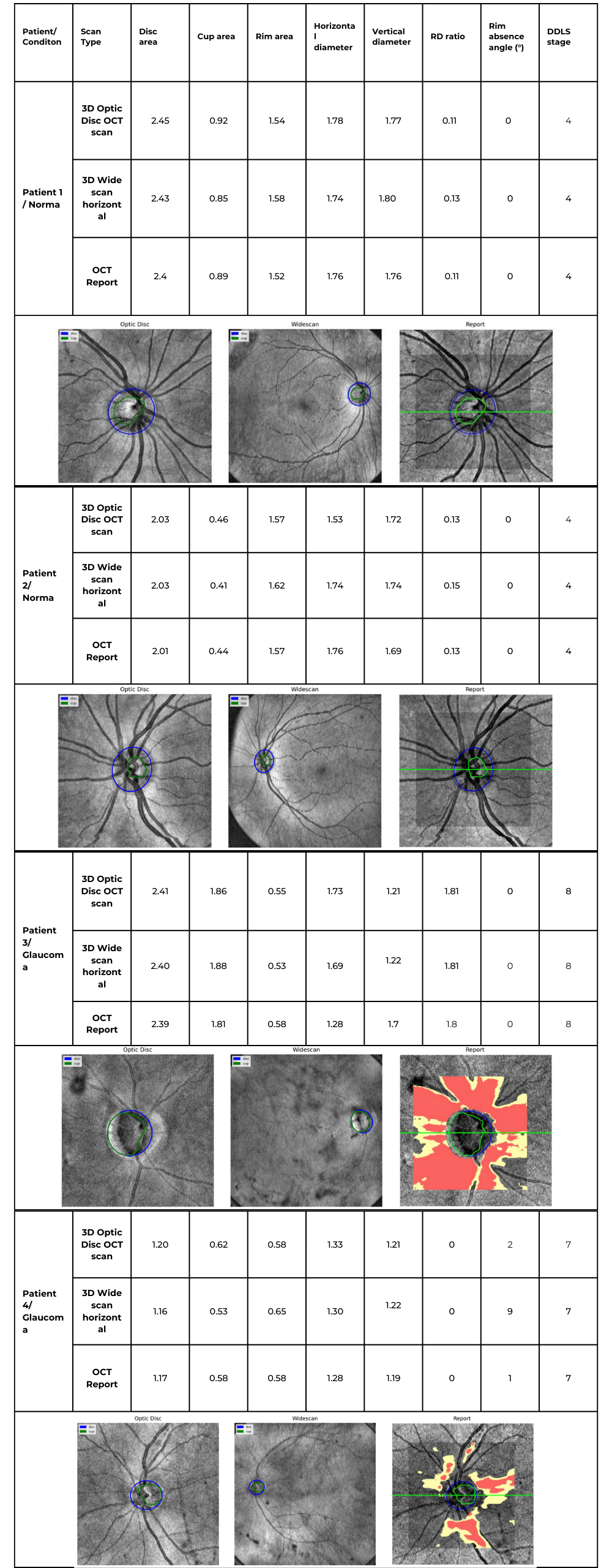
2.3. Patient Case Studies: DDLS Analysis in Real-World Scenarios
Accurate assessment of glaucoma severity relies on precise measurements of optic nerve parameters, such as disc area, rim-to-disc ratio, and rim absence angle. In the following examples, we analyzed four patient cases, including both normal optic discs and glaucomatous eyes, using 3D Optic Disc OCT scan, 3D Wide scan OCT, and device-generated reports as a reference standard.
By consolidating individual patient cases into a single comparative table, we can examine the consistency of DDLS analysis across different scan types and highlight key variations that may arise due to differences in scan coverage, segmentation accuracy, and anatomical structure. The following table summarizes the key optic nerve parameters measured for each patient and scan type.

Table 2. Comparative DDLS Evaluation Across Multiple Patient Cases
Key Findings & Interpretation
1. High Consistency Between Our Method and Device Reports
- Across all cases, the DDLS stage remains identical (4 for normal eyes, 7 or 8 for glaucomatous cases) regardless of whether the input scan was 3D Optic Disc OCT or wide scan, and this result corresponds to the device-generated report.
- Key optic nerve parameters such as disc area, cup area, and rim area closely align with the device reference, demonstrating strong algorithm performance.
2. Minor Variations in Cup and Rim Measurements
- Cup and rim area values show slight deviations between 3D Optic Disc OCT scans and 3D Wide scan scans, which is expected due to differences in scan coverage and segmentation sensitivity.
- For example, in Patient 3 (Glaucoma, Stage 8):
- Cup area was 1.86 mm² (3D Optic Disc OCT scan), 1.88 mm² (3D Wide scan), and 1.81 mm² (Device Report).
- Rim area was 0.55 mm² (3D Optic Disc OCT scan), 0.53 mm² (3D Wide scan), and 0.58 mm² (Device Report).
- These small variations do not affect final DDLS staging but highlight how scan type can introduce subtle segmentation differences.
3. Rim Absence Angle Varies Slightly but Remains Within Expected Tolerances
- The rim absence angle shows minor fluctuations across scan types, especially in glaucomatous cases.
- Example: In Patient 3 (Stage 8 Glaucoma), the device reported a rim absence angle of 162°, while our algorithm calculated 155° (3D Optic Disc OCT scan) and 151° (3D Wide scan).
- Since DDLS categories for severe glaucoma are defined in large increments (e.g., 45°+ thresholds), these small differences do not impact staging accuracy.
4. 3D Wide scan OCT Provides Comparable Results to 3D Optic Disc OCT scan
- Despite covering a larger field of view, wide scans produced DDLS staging results consistent with 3D Optic Disc OCT scans and device reports.
- In patients with coexisting macular pathologies, 3D Wide scan OCT may provide additional clinical insights while still maintaining high reliability for glaucoma staging.
Conclusion: Reliable DDLS Analysis Across Different Scan Types
This unified case study analysis confirms that our DDLS analysis algorithm produces highly consistent results across different scan protocols and patient conditions.
- DDLS stage assignment is identical to device reports across all scan types, ensuring high agreement with clinically validated reference values.
- Key optic nerve measurements (disc area, cup area, rim area) are closely aligned across 3D Optic Disc OCT scan, 3D Wide scan, and device reports, reinforcing algorithm accuracy.
- Minor variations in rim absence angle and segmentation metrics do not affect final glaucoma staging, highlighting the algorithm’s robustness.
- 3D Wide scan OCT offers a viable alternative for 3D Optic Disc OCT scans, particularly in cases where both macular and optic nerve regions need simultaneous evaluation.
5. Visual Comparison Shows Strong Similarity to Device Reports
- The disk and cup boundaries detected by our algorithm closely match those in the device-generated reports, maintaining consistent shapes and anatomical alignment across both 3D Optic Disc and 3D Wide scan OCT scans.
- However, wide scan-based segmentations tend to be slightly rougher, as less structural information is available compared to dedicated optic disc scans. This trade-off is expected due to the broader field of view in wide scans.
These findings validate our algorithm’s flexibility, adaptability, and clinical reliability, demonstrating its potential for seamless integration into real-world ophthalmic workflows.
2.4. Why Our Approach Stands Out: Key Advantages Over Traditional DDLS Systems
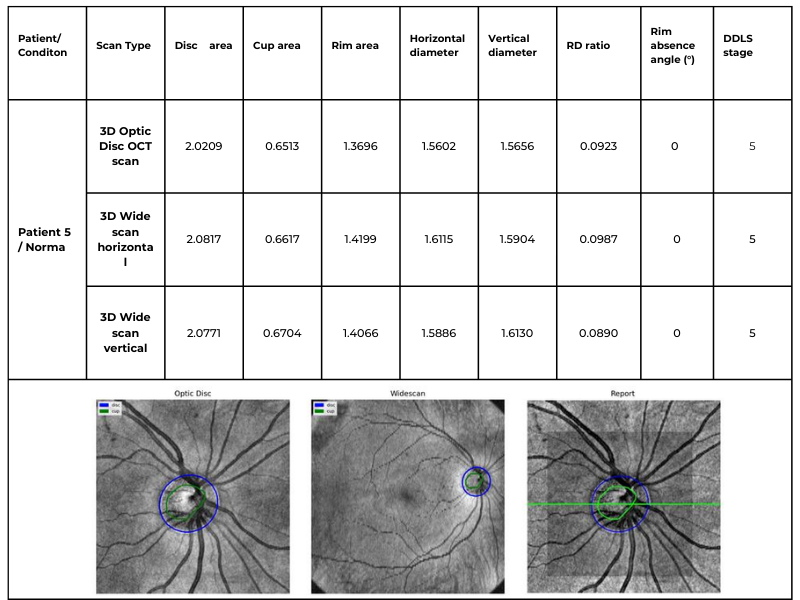
While the previous patient case studies demonstrated the accuracy and consistency of our DDLS analysis across different optic disc conditions, another critical advantage of our method is its ability to work seamlessly across various scanning protocols. Unlike traditional device-restricted solutions, our approach supports DDLS assessment on both standard 3D Optic Disc OCT scans and 3D Wide scans with different orientations.
The following table illustrates the same patient’s optic nerve head analyzed using three different scanning protocols: 3D Optic Disc OCT scan, 3D Wide scan Horizontal, and 3D Wide scan Vertical. This comparison highlights the method’s adaptability to different scan formats, ensuring reliable DDLS analysis regardless of the scanning protocol used. This example is taken from a Topcon Maestro 2 OCT system, providing an additional reference for processing across different OCT systems.

Table 3. Comparative DDLS Analysis Across Different Scanning Protocols: 3D Optic Disc OCT, 3D Wide scan Horizontal, and 3D Wide scan Vertical.
This capability significantly enhances clinical applicability, allowing our algorithm to process data from various scanning protocols and devices while maintaining high accuracy. The ability to analyze both 3D Optic Disc and 3D Wide scan OCT scans — across different orientations and machine types — ensures comprehensive glaucoma assessment even in cases where scan availability or quality may vary.
Key advantages over traditional DDLS analysis methods
1. Device Independence
- While most existing solutions are restricted to proprietary OCT data formats, our algorithm processes scans from any OCT system, ensuring broad compatibility across devices.
2. Consistent Accuracy Across Different Scan Types
- Our algorithm closely matches device-generated DDLS reports, achieving 97.3% accuracy for 3D Optic Disc OCT scans and 94.59% for 3D Wide scan OCTs.
- Patient cases confirm this consistency, with both normal and glaucomatous eyes correctly classified, even when analyzed with different scan types.
3. Robust Performance in Edge Cases
- Unlike traditional device-based DDLS assessments, which may struggle with low-quality images or atypical anatomical features, our approach maintains high accuracy in challenging clinical scenarios.
- Patient examples with small optic discs and advanced-stage glaucoma demonstrated that our algorithm successfully identified key DDLS indicators even when scan quality or nerve structure was less distinct.
4. Expanded Assessment Through 3D Wide scan OCT
- The ability to perform DDLS analysis on Horizontal and Vertical 3D Wide scans allows for a more comprehensive evaluation by incorporating both macular and optic nerve data.
- In patients with coexisting macular pathologies, wide scans enabled earlier detection of glaucomatous changes that would have been missed if only optic disc scans were used.
3. Detailed Approach Description
To assess glaucoma stage on OCT scans using DDLS analysis, the following steps should be performed:
- Optic Nerve Landmarks Detection – Localization of the optic nerve in the b-scan view of each scan by identifying key anatomical landmarks.
- ILM Detection – Segmentation of the inner limiting membrane (ILM) in the b-scan view of each scan to establish a reference for neuroretinal rim measurement.
- Neuroretinal Rim Reconstruction – Construction of the neuroretinal rim geometry based on detected nerve landmarks and ILM segmentation.
- DDLS Analysis – Application of the Disc Damage Likelihood Scale (DDLS) to assess glaucoma severity based on neuroretinal rim measurements. This includes assigning a DDLS stage according to rim width and optic disc size, with a focus on detecting localized thinning and asymmetry.
3.1. Keypoint Annotation Process / Nerve Detection
The foundation of our approach lies in a high-quality, annotated dataset meticulously labeled by a team of four expert ophthalmologists. The annotation process focused on identifying key anatomical landmarks in both the macular region and the optic disc nerve zones, both of which are critical for detecting glaucomatous changes and performing Disc Damage Likelihood Scale (DDLS) analysis.
These keypoints serve as essential data for evaluating disease progression and training machine learning models. The dataset was carefully selected based on key clinical features, such as the presence or absence of nerve fibers, foveal pits, and other pathological markers, ensuring a comprehensive representation of various conditions and scan types.
The annotated dataset consists of approximately 370 unique OCT examinations with more than 56,000 b-scans, covering a range of physical scanning areas, pathology types, and optic nerve conditions to enhance the model’s robustness. The scans are categorized as follows:
- Optic Disc with no excavation: ~15 examinations;
- Glaucomatous Optic Disc: ~105 examinations;
- Normal Optic Disc: ~105 examinations;
- Wide scans (covering both the macular and optic nerve regions): ~60 examinations;
- Normal Retina Scans: ~40 examinations;
- Pathological Retina Scans: ~45 examinations.
This detailed annotation process ensures high precision and reliability, enabling the algorithm to generalize across diverse cases while maintaining clinical accuracy in real-world scenarios.
3.2. Eye Keypoints Retrieval / OCT Keypoint Detector
Our keypoint detection model represents a logical evolution of the model for exam center detection, designed to efficiently and accurately identify key anatomical landmarks in OCT scans. The architecture integrates elements from UNet 5 and CenterNet 6, incorporating YOLO-inspired 7 techniques for keypoint prediction. Additionally, the backbone has been adapted to a transformer-based model 8, enhancing feature extraction capabilities.
Training Process
The training process follows a multi-stage approach, ensuring robustness, accuracy, and efficiency:
- Stage 1: Detects general keypoints, establishing a foundation for precise landmark localization.
- Stage 2: Groups and refines the identification of specific keypoints, progressively improving the model’s understanding of anatomical structures.
This structured approach enhances the model’s reliability across different scan types while maintaining computational efficiency.
Key Features
Data Preprocessing
- The data is augmented using unsupervised techniques, leveraging libraries such as Albumentations 9 to introduce variations such as rotations, scaling, and noise addition.
- This ensures the model encounters a wider variety of real-world scenarios during training, improving its generalization capability.
Training Process
- The model is trained using supervised learning techniques, optimizing a loss function through backpropagation and gradient descent.
- This approach allows for continuous refinement and adaptation to complex variations in OCT scans.
Parameterization & Tuning
- The model includes millions of adjustable parameters (weights), which are fine-tuned to increase accuracy.
- Key hyperparameters such as learning rate, batch size, and network depth are carefully selected to maximize performance.
- Advanced optimization techniques, including grid search, random search, and Bayesian optimization, are used to find the best hyperparameter configuration.
3.3. Retina Layers Segmentation Model
The Retina Layers Segmentation Model is our production-stage model, actively used within the Altris AI platform. It was incorporated into this experiment without modifications, ensuring that the results reflect real-world performance as seen in our deployed system.
Our Retina Layers Segmentation Model enables precise segmentation of key retinal layers in OCT scans, crucial for detecting structural changes linked to glaucoma and other retinal diseases. The model identifies:
- ILM, RNFL, GCL, IPL, INL, OPL, ONL, ELM, MZ, EZ, OS, RPE, BM
The training dataset consists of 5,000 expert-annotated OCT b-scans, covering a diverse range of patient demographics, including different ages and ethnic backgrounds. The segmentation model is designed to detect and delineate key retinal layers with high accuracy.
Training & Architecture
The model is based on U-Net with a ResNet backbone, optimized for OCT images. Training includes:
- Expert Annotation: Medical specialists labeled layers for ground truth.
- Augmentation: Albumentations-based transformations enhance robustness.
- Supervised Learning: Predicts segmentation masks using backpropagation.
- Hyperparameter Optimization: Grid search, random search, and Bayesian tuning maximize performance.
Model Validation & Performance
- The model was validated using a holdout validation approach, with separate validation and test sets that were not exposed during training.
- Real-world testing was conducted using scans from various clinical settings to ensure robustness.
- Performance was evaluated using the Mean Dice Coefficient across all layers, achieving a score of 0.80, with layer-specific scores ranging from 0.63 to 0.92, confirming high segmentation accuracy.
- Cross-domain testing demonstrated consistent performance across different OCT systems, and stability was confirmed over scans collected across different time periods.
This efficient, accurate, and generalizable model strengthens DDLS analysis and enhances AI-driven retinal diagnostics.
3.4. DDLS Algorithm
The DDLS algorithm evaluates glaucomatous changes by analyzing the geometric relationship between the neural rim and optic cup in the optic nerve head. Key steps include:
- Localization: Identifying boundaries of the optic cup and neuroretinal rim by reconstructing geometry on a b-scan view using disc landmarks and an inner limiting membrane.

Figure 5. B-scan Geometry Visualization.
- Measurement: Calculating the DDLS stage based on the ratio between the rim and disc boundaries.
- Cross-Scan Application: Adapting the analysis for 3D Wide scans (both Horizontal and Vertical protocols) as well as 3D Optic Disc-specific scans.
Our implementation enhances this traditional method by leveraging wide scans, enabling a more comprehensive assessment of glaucomatous changes.
3.5. Evaluation
To ensure the reliability and effectiveness of our DDLS algorithm, we conducted a rigorous evaluation process, adhering to best practices in data usage, ethics, and performance validation.
Data Integrity
- Measures were implemented to prevent data leakage, ensuring that scans from the same patient did not appear in both training and testing sets.
Ethical Considerations
- The analysis strictly relies on OCT-related data (e.g., scan zone size, laterality, pixel spacing) without incorporating any personal patient information.
Performance Metrics
- Keypoint detection accuracy was evaluated using Mean Squared Error (MSE), comparing model-predicted keypoints with expert annotations.
- Additional metrics included correctness of scan center-related landmarks and accuracy in the optic nerve region, ensuring precision in clinical applications.
The evaluation results confirmed the algorithm’s robustness, demonstrating significant performance gains, particularly in edge cases, where traditional methods often struggle.
Discussion
Our DDLS analysis method represents a significant advancement in glaucoma detection. Key benefits include:
- Universal Compatibility: The ability to process data from various devices ensures broad applicability.
- Enhanced Accuracy: By incorporating data from both macular and optic nerve regions, our approach captures more subtle glaucomatous changes.
- Edge Case Performance: Advanced machine learning techniques enable accurate analysis even in challenging scenarios.
Compared to traditional methods, our system provides a more flexible, reliable, and comprehensive solution for early glaucoma detection.
FDA-cleared AI for OCT analysis
Conclusion
By integrating 3D Wide scans and state-of-the-art machine learning models, we have enhanced DDLS analysis for glaucoma detection, ensuring high accuracy, broad compatibility, and robustness across diverse clinical scenarios.
Unlike traditional solutions, our algorithm:
- Works across multiple OCT devices, eliminating the constraints of proprietary data formats.
- It closely matches device-generated DDLS reports, achieving 97.3% accuracy for 3D Optic Disc OCT scans and 94.59% for 3D Wide scans.
- Performs reliably in edge cases, such as small optic discs and advanced-stage glaucoma, where traditional methods may struggle.
- Supports both Horizontal and Vertical 3D Wide scans, enabling more comprehensive assessments that incorporate both macular and optic nerve data.
- Enhances early glaucoma detection, particularly in patients with coexisting macular pathologies, where wide scans provide additional clinical insights.
By delivering consistently accurate DDLS staging, regardless of scan type or manufacturer, our system establishes a new benchmark for universal glaucoma assessment. This technology has the potential to significantly improve early detection and management, ultimately preserving vision and enhancing patient outcomes.
References
- Spaeth, G. L. (2005). The Disc Damage Likelihood Scale. Glaucoma Today. https://glaucomatoday.com/articles/2005-jan-feb/0105_18.html
- Cheng, K. K. W., & Tatham, A. J. (2021). Spotlight on the Disc-Damage Likelihood Scale (DDLS). Clinical Ophthalmology, 15, 4059–4071. https://pmc.ncbi.nlm.nih.gov/articles/PMC8504474/
- Zangalli, C., Gupta, S. R., & Spaeth, G. L. (2011). The disc as the basis of treatment for glaucoma. Saudi Journal of Ophthalmology, 25(4), 381-387. https://www.sciencedirect.com/science/article/pii/S1319453411000993
- Review of Optometry Staff. (2023, January 23). Optic disc staging systems effective in grading advanced glaucoma. Review of Optometry. https://www.reviewofoptometry.com/article/optic-disc-staging-systems-effective-in-grading-advanced-glaucoma
- Ronneberger O, Fischer P, Brox T. U-Net: Convolutional Networks for Biomedical Image Segmentation. [Preprint]. Posted May 18, 2015. https://arxiv.org/abs/1505.04597
- Duan K, Bai S, Xie L, et al. CenterNet: Keypoint Triplets for Object Detection. [Preprint]. Posted April 17, 2019. https://arxiv.org/abs/1904.08189
- Redmon J, Divvala S, Girshick R, Farhadi A. You Only Look Once: Unified, Real-Time Object Detection. [Preprint]. Posted June 8, 2015. https://arxiv.org/abs/1506.02640
- Dosovitskiy A, Beyer L, Kolesnikov A, et al. An Image is Worth 16×16 Words: Transformers for Image Recognition at Scale. [Preprint]. Posted October 22, 2020. https://arxiv.org/abs/2010.11929
- Buslaev A, Iglovikov V, Khvedchenya E, et al. Albumentations: Fast and Flexible Image Augmentations. [Preprint]. Posted September 18, 2018. https://arxiv.org/abs/1809.06839
-
Altris AI Introduces Next-Generation Fluids and GA Quantification Features
Maria Znamenska, MD, PhD Ophthalmology
1 min. readAltris AI Introduces Next-Generation Fluids and GA Quantification Features
Altris AI, a pioneering force in artificial intelligence for OCT scan analysis, has unveiled additional quantification features for Fluids and Geographic Atrophy (GA) tracking on its web platform. Altris AI currently detects over 70 retina pathologies and biomarkers. However, we have decided to enhance its capabilities by adding additional Fluids and GA quantification and tracking functionalities, recognizing that eye care specialists frequently work with these conditions.
These advancements empower eye care professionals (ECPs) with cutting-edge tools for diagnosing and managing retinal diseases. By integrating AI-driven quantitative tracking and progression monitoring, Altris AI enables specialists to deliver more personalized and effective treatments, ultimately enhancing patient outcomes.
Fluids Quantification and Progression Tracking
The presence of fluids such as Intraretinal Cystoid Fluid (IRC), Diffuse Edema, Subretinal Fluid (SRF), and Serous Retinal Pigment Epithelium (RPE) Detachment are critical biomarkers for conditions like nAMD, DME, DR, and RVO. Accurate detection, quantification, and tracking of these fluids are essential for monitoring disease activity, evaluating treatment efficacy, and making informed prognoses.
We created specialized more detailed functions which detect these biomarkers for more specific and accurate tracking. The AI algorithm was additionally trained to work directly with fluids taking into account the importance of these biomarkers for accurate diagnostics.
Altris AI’s advanced algorithms, trained on millions of OCT scans, provide precise and objective fluid analysis. Each of the four fluid types is localized and color-coded for clarity. Quantitative metrics such as volume, area, and ETDRS grids (1, 3, and 6 mm) are calculated and presented in mm3 or nanoliters for comprehensive evaluation. The Progression Tracking feature offers historical trend analysis with intuitive visualizations through graphs and percentages. For instance, if Cystoid Fluid (IRC) increases in volume, ECPs can immediately identify and address the change.

Precision in Geographic Atrophy (GA) Monitoring
Recent advancements in GA treatment have led to a growing need for large-scale screening in clinical practice. However, this increased demand often means higher workloads and less time for in-depth analysis.
The platform facilitates automated detection, quantification, and tracking of GA by analyzing key biomarkers: Pigment Epithelium (RPE) atrophy, Hypertransmission, Neurosensory Retina Atrophy, and Ellipsoid Zone (EZ) disruption. These biomarkers are color-coded for easier identification.
We assess GA using three key criteria:
- Overlapping region of 3 biomarkers: Hypertransmission, RPE Atrophy, and Neurosensory Retina Atrophy (referred as the GA zone).
- The shortest distance from the Fovea center to the GA zone.
- Percentage of the GA zone covering the 1 mm, 3 mm, and 6 mm ETDRS grid areas.
We also improved the accuracy of a critical step in our AI pipeline: the fovea and central scan detection. Altris AI’s updated model is much more robust in detecting fovea zone and central scan now. Especially in cases when the center cannot be distinguished due to pathology presence or other reasons, the model is trained to analyze the whole surface and find reference locations from which a central scan could be determined. The new model can find an accurate center in 95% of cases, in other situations, it can efficiently estimate the center location (as opposed to a simple analysis flow used by ECPs where the geometrical center is selected). This advancement significantly enhances the precision of GA detection.
Further Progression Tracking enhances GA management by visualizing changes over time, supporting timely and accurate treatment decisions. By streamlining workflows and providing actionable insights, this feature helps ECPs make informed choices and potentially preserve vision in GA patients.
Dr. Maria Znamenska, MD, PhD, and a Chief Medical Officer at Altris AI, commented:
“We listened to our clients and introduced Fluids and GA tracking features. In 2025, eye care specialists will have the tools to combine their expertise with next-generation AI technology to effectively tackle conditions that threaten vision. Our formula is simple: detect, quantify, and track fluids, GA, and 70+ retina pathologies and biomarkers for better patient outcomes.”
About Altris AI
Altris AI is an artificial intelligence platform for OCT analysis that detects the widest range of retina pathologies and biomarkers on the market – more than 70. Leading the way in AI innovation, Altris AI provides transformative solutions that enhance the diagnosis, treatment, and monitoring of retinal diseases, enabling eye care professionals to deliver exceptional patient care.
-
OCT Scan Normal Eye vs 8 Most Common Pathologies
Maria Znamenska
31.10.202414 min readOCT Scan Normal Eye vs. 8 Most Common Pathologies
Differentiating between an OCT scan of a normal eye vs. a pathological one is a practical skill gained after years and years of practice. However, educating yourself on the basic differences will speed up the process. Understanding the “why” and “how” behind any changes on the OCT scan, compared to a normal macula OCT, will speed up your learning curve and deepen your expertise as a retinal expert.
FDA-cleared AI for OCT analysis
The article’s first part focuses on key OCT features and their meaning as a structural change for retinal architecture. The second part discusses the most recognizable OCT features of eight common pathologies.
OCT Scan: Normal Eye
When evaluating an OCT scan, the most logical step is to understand how a normal macula OCT should look. The most telling feature across all scans is the contrast between light and dark areas. Typically, the nerve fiber layer and the underlying ganglion cell layer appear brighter than the densely packed nuclear layers. This is followed by the inner plexiform layer interface, which presents as a bright, hyperreflective area.
The inner nuclear layer, composed of densely packed nuclei, appears dark. This is followed by the outer plexiform layer, the outer nuclear layer, and Henle’s layer. The external limiting membrane, an important landmark for assessing retinal health, is also visible. The ellipsoid zone (EZ) is another bright layer, while the interdigitation zone may not always be distinguishable from the underlying RPE layer, even in healthy eyes. Finally, the RPE and inner choroid appear hyperreflective.
Structure
The ELM and EZ are critical structures to assess. In a normal macula OCT, the distance between the EZ and ELM is shorter than between the EZ and the RPE. The apparent “elevation” of the EZ in the foveal center results from the elongated outer segments of the foveal cones.
It’s important to remember that not all retinal structures are readily visible on a normal macula OCT. For example, Henle’s fiber layer is more easily distinguished in the presence of retinal pathology, such as swelling or thinning. Similarly, Bruch’s membrane is usually not visualized unless there is a separation between the RPE and Bruch’s membrane, often indicative of disease.
Thickness
Choroidal thickness is another key factor in OCT assessment. A general rule of thumb is that the choroid (between the RPE and the outer choroidal boundary) is approximately as thick as the retina. Thinning of the choroid may be observed in myopic or older patients, while marked choroidal thickening can raise suspicion for diseases like central serous retinopathy.
The OCT scan also provides information about laterality. The nerve fiber layer is characteristically thicker near the optic nerve head. Conversely, if the nerve fiber layer is not visualized in its expected location on an otherwise OCT normal scan, it could signal significant nerve fiber layer loss, potentially due to glaucoma or other optic neuropathies.
Reflectivity
Specific OCT terminology helps describe scans and differentiate normal findings from pathology.
Two fundamental concepts in OCT interpretation are hyporeflectivity and hyperreflectivity, which form the basis for understanding the structural composition of the retina as visualized in an OCT scan.
FDA-cleared AI for OCT analysis
Hyporeflectivity refers to the increased light transmission capacity of a structure. The OCT scanning laser beam passes through hyporeflective structures with minimal reflection. The quintessential example of a hyporeflective structure is the vitreous humor. It appears as a dark area in the uppermost portion of a normal OCT scan, situated above the retina.
But hyporeflectivity can also be pathological, deviating from the patterns observed in a normal macula OCT; in the retina, it manifests in three primary ways.
Like the vitreous, subretinal fluid exhibits high light transmission and appears black on OCT. A uniformly black region suggests the fluid lacks cellular debris or other inclusions.
Subretinal fluid on OCT
Fluid can also accumulate within the retinal layers, for example, between the layers of the neuroepithelium. This intraretinal fluid also appears hyporeflective on OCT.
Intraretinal fluid on OCT
Following a degenerative process within the retina, a cavity or void may form where retinal tissue has been lost. These degenerative cavities lack the cellular components necessary to reflect light and thus appear as dark spaces on OCT. It’s important to differentiate these cavities from cystic spaces, which may have distinct clinical implications.
One example is outer retinal tubulations. While associated with various diseases, outer retinal tubulations (ORTs) generally indicate outer retinal degeneration and atrophy.
Outer retinal tubulations on OCT
Hyperreflectivity, unlike hyporeflectivity, indicates structures with high light reflectance. On the grayscale spectrum of an OCT image, hyperreflective structures appear progressively whiter.
The retinal pigment epithelium (RPE) complex and Bruch’s membrane are considered the most hyperreflective structures in a normal macula OCT.
Pathological processes can introduce new hyperreflective elements within the retina, aiding in differentiating normal and abnormal OCT scans. A typical example is hard exudates, frequently observed in diabetic retinopathy. These lipid-rich deposits are extremely dense, causing them to appear bright white on OCT due to the complete reflection of incident light. Furthermore, this high density leads to a shadowing effect beneath the deposits, caused by strong backscattering of the OCT signal.
Hard exudates and shadowing on OCT
Epiretinal membranes (ERMs) – a thin membrane or layer of scar tissue that forms over the retina – are also hyperreflective. It is composed of dense connective tissue with high light-reflecting properties and appears white on OCT scans.
FDA-cleared AI for OCT analysis
Integrity
Beyond hypo- and hyperreflectivity, OCT interpretation involves assessing the structural integrity of retinal layers. For instance, in an OCT scan of a normal eye, Bruch’s membrane appears as a thin, continuous line underlying the retinal pigment epithelium (RPE). The RPE is a monolayer of cells, ideally presenting with a smooth and uniform optical density. However, some pathologies, particularly early stages of age-related macular degeneration (AMD), may show unevenness or integrity loss in the RPE and Bruch’s membrane complex.
Disruption of the ellipsoid zone (EZ) is a particularly concerning finding on OCT, often indicating photoreceptor damage. Significant disruption of the EZ in the central macula is a strong biomarker for adverse visual outcomes.
The closer the loss of integrity extends toward the foveal center, the poorer the visual prognosis tends to be.
Ellipsoid zone disruption on OCT
OCT also plays a crucial role in visualizing and characterizing breaks in the structural integrity of the retina. These breaks, commonly referred to as retinal tears or holes, can be classified as full-thickness or partial-thickness, depending on the extent of retinal involvement.
Full-thickness breaks completely separate all retinal layers, while partial-thickness breaks involve only some retinal layers. OCT allows for precise delineation of the layers involved and the overall morphology of the break.
Retinal holes can also be categorized by their location. Macular holes, as the name suggests, involve the central retina and can lead to significant central vision loss and require prompt attention.
Lamellar macular hole on OCT
Non-macular holes occur outside the central macular region, often in the peripheral retina. While they may not cause immediate central vision disturbances, they can still lead to serious complications, such as retinal detachment, if left untreated.
Definition
The blurring of retinal structures, or loss of definition, is another key OCT concept. This loss of the retina’s normal layered organization, seen in diseases like AMD, manifests as indistinct layers merging into a homogenous mass.
Disorganisation of retinal inner layers on OCT
Hypertransmission in OCT refers to enhanced signal penetration due to reduced blockage of the OCT light signal. This phenomenon is frequently observed in geographic atrophy, a late stage of AMD characterized by the atrophy of the retinal pigment epithelium, choriocapillaris, and photoreceptors.
Hypertransmission on OCTIn a normal macula OCT, a signal is attenuated as it traverses the various retinal layers, with a portion of the signal being reflected to the detector. However, in geographic atrophy (GA), the loss of RPE and other retinal structures reduces this attenuation, allowing the OCT signal to penetrate deeper into the choroid. This increased penetration results in a stronger signal return from the choroidal layers, creating essentially a “corridor” of enhanced signal penetration through the atrophic areas of the retina. This deep penetration and strong signal return, unfortunately, indicate significant retinal damage and are associated with a poor visual prognosis.
Displacement
Another term used to describe OCT scan results is elevation. It refers to the upward displacement of retinal structures from their normal anatomical position. In the context of age-related macular degeneration (AMD), elevation is frequently associated with the presence of drusen.
Drusen are extracellular deposits that accumulate between the retinal pigment epithelium (RPE) and Bruch’s membrane. They are a hallmark of AMD and can vary in size, shape, and composition. Drusen are typically categorized as hard, soft, or confluent based on their ophthalmoscopic appearance.
Hard and soft drusen on OCT
In contrast to elevation, depression in OCT describes the inward displacement or concavity of retinal structures. This can be a manifestation of various pathological processes, with a prominent example of degenerative myopia.
Degenerative myopia on OCT
OCT scan: normal eye transformation through pathologies
Age-related macular degeneration (AMD)
AMD is an acquired degenerative macular disease usually affecting individuals over the age of 55 years. It is characterized by pathologic alterations of the outer retina, retinal pigment epithelium (RPE), Bruch’s membrane, and choriocapillaris complex, including drusen formation and pigmentary changes.
AMD is a progressive disease, and in advanced stages, central geographic atrophy and neovascularization, may develop and reduce vision. OCT plays a critical role in distinguishing between the different stages and forms of AMD, particularly when compared to the features of an OCT normal scan.
Wet AMD
Neovascular or “wet” age-related macular degeneration (nAMD) arises from the aberrant growth of choroidal vessels that penetrate Bruch’s membrane and invade the subretinal space. These abnormal vessels leak fluid and blood, disrupting the retinal architecture and causing vision loss.
Several key OCT features can signal the presence and activity of nAMD in comparison to a normal OCT scan:
- Fluid Accumulation: The presence and location of fluid are hallmarks of nAMD (hence the term ‘wet AMD’). Intraretinal fluid, appearing within the retinal layers, often signifies more severe disease and a poorer visual prognosis than subretinal fluid, which accumulates beneath the retina.
- RPE Detachment: Serous PED appears as a dome-shaped elevation of the RPE due to fluid accumulation beneath it. PEDs often accompany nAMD and can vary in size and shape.
- Disruption of Retinal Layers: nAMD can disrupt the normal retinal architecture, particularly the photoreceptor layer. Damage to the ellipsoid zone (EZ) and external limiting membrane (ELM) is visible on OCT and correlates with visual impairment.
- Hyperreflective Foci: Hyperreflective dots (HRDs) are small, bright spots scattered throughout the retina.
- Subretinal Hyperreflective Material (SHRM): Appears as a hyperreflective band between the retina and RPE. Its composition varies but may include fluid, fibrin, blood, and neovascular tissue; it can be associated with poorer visual outcomes.
- RPE Tears: These are disruptions in the RPE monolayer, often occurring in areas of PED. RPE tears can lead to significant vision loss and are an important complication of nAMD.
- Choroidal Changes: nAMD can also affect the choroid, the vascular layer beneath the RPE.
Dry AMD
In its early stages, Dry AMD is characterized by drusen and pigmentary abnormalities resulting from alterations in the retinal pigment epithelium (RPE). Later, it can progress to geographic atrophy (GA) or outer retinal atrophy.
The three classic findings in Dry AMD are drusen, pigmentary changes, and geographic atrophy.
Drusen are classified as:
- small (<65 um),
- medium (65 – 124 um),
- or large (>125 um).
While both drusen and pigmentary changes can appear as yellowish deposits in the retina, pigmentary changes are often more varied in color (ranging from yellow to brown or black) and less defined in shape than the generally circular drusen.
Geographic atrophy typically begins in the paracentral macula, often surrounding the fovea in a horseshoe pattern. It can eventually involve the fovea itself, leading to severe vision loss.
Diabetic Retinopaty (DR)
Diabetic retinopathy (DR), a leading cause of vision loss in working-age populations, is characterized by retinal vascular abnormalities. It progresses from non-proliferative DR (NPDR), marked by vascular leakage and capillary occlusion, to proliferative DR (PDR), where neovascularization can lead to severe vision impairment through vitreous hemorrhage or retinal detachment.
OCT can aid in identifying the earliest sign of DR: microaneurysms. They appear as small, distinct, oval-shaped, hyperreflective, walled structures associated with microvascular damage. Specifically, the structural weakness of the vessel wall of MAs causes fluid leakage, resulting in edema.
Another consequence of microaneurysm formation is the progression to intraretinal hemorrhages (IRH), often called ‘dot-blot’ hemorrhages. These appear as hyperreflective foci on OCT cross-sections, with varying degrees of opacification.
Diabetic macular edema (DME) can occur at any stage of the disease and is the most common cause of vision loss in those with diabetes. It results from a blood-retinal barrier breakdown, leading to fluid leakage and retinal thickening.
Retinal vein occlusions
Retinal vein occlusions (RVOs) are blockages of the retinal veins responsible for draining blood from the retina. These blockages can affect either the central retinal vein (CRVO) or one of its branches (BRVO). RVOs are more prevalent in older individuals and those with underlying vascular conditions such as high blood pressure, high cholesterol, a history of heart attack or stroke, diabetes, or glaucoma. The primary vision-threatening complications of RVO are macular edema, which involves fluid accumulation in the central retina, and retinal ischemia, which results from insufficient blood flow to the retina.
While both Central Retinal Vein Occlusion (CRVO) and Branch Retinal Vein Occlusion (BRVO) involve blockage of a retinal vein, the underlying cause and location of the blockage differ.
CRVO occurs when a thrombus (blood clot) blocks the central retinal vein near the lamina cribrosa, where the optic nerve exits the eye.
In contrast, BRVO typically occurs at an arteriovenous crossing point, where a retinal artery and vein intersect. Atherosclerosis (hardening of the arteries) can compress the vein at this crossing point, leading to thrombus formation and occlusion.
In CRVO, the retina often exhibits extensive intraretinal hemorrhages, dilated and tortuous veins, and cotton-wool spots. This constellation of findings is classically described as a “blood and thunder” appearance. In BRVO, the signs are typically localized to the area of the retina drained by the affected vein. Macular edema, characterized by retinal thickening and cystoid spaces within the retina, is a common finding in CRVO and BRVO and can significantly contribute to vision loss.
Central serous retinopathy
Central serous chorioretinopathy (CSCR) is a common retinal disorder that causes visual impairment and altered visual function. It is classified as a pachychoroid disease, including conditions like polypoidal choroidal vasculopathy and pachychoroid neovasculopathy.
OCT imaging in CSCR often reveals a thicker-than-average choroid.
This diagnostic is particularly useful in cases where clinical examination findings are inconclusive, distinguishing subtle differences between normal and abnormal OCT scans in terms of structural changes, such as small pigment epithelial detachments (PEDs) and hyperreflective subretinal fluid, that may not readily appear on clinical exams.
Furthermore, OCT is valuable for monitoring disease progression and resolution in chronic CSCR cases. A distinguishing feature that can also be seen in CSR is the appearance of the retinal pigment epithelium: the RPE line typically appears straight in non-affected areas, while it can appear wavy or irregular in areas with CSCR.
Epiretinal membrane (Epiretinal fibrosis)
Epiretinal fibrosis (epiretinal membrane/macular pucker) is a common condition affecting the central retina, specifically the macula. It is characterized by a semi-translucent, avascular membrane that forms on the retinal surface, overlying the internal limiting membrane (ILM), which is absent on a normal macula OCT.
OCT plays a crucial role in assessing the severity of ERMs, revealing the extent of macular distortion and the involvement of retinal layers.
OCT findings in ERMs are used to stage the severity of the membrane, ranging:
- Stage 1: ERMs are mild and thin. Foveal depression is present.
- Stage 2: ERMs with widening the outer nuclear layer and losing the foveal depression.
- Stage 3: ERMs with continuous ectopic inner foveal layers crossing the entire foveal area.
- Stage 4: ERMs are thick with continuous ectopic inner foveal and disrupted retinal layers.
Retinal detachment
Retinal detachment is an important cause of decreased visual acuity and blindness, a common ocular emergency often requiring urgent treatment.
It occurs when subretinal fluid accumulates between the neurosensory retina and the retinal pigment epithelium through three mechanisms:
- Rhegmatogenous: a break in the retina allowing liquified vitreous to enter the subretinal space directly.
- Tractional: proliferative membranes on the surface of the retina or vitreous pull on the neurosensory retina, causing a physical separation between the neurosensory retina and retinal pigment epithelium
- Exudative: accumulation of subretinal fluid due to inflammatory mediators or exudation of fluid from a mass lesion/insufficient RPE function
OCT helps identify foveal status and diagnose tractional or exudative retinal detachments, aiding in treatment planning.
Macular hole
Macular holes are full-thickness defects of retinal tissue involving the anatomic fovea and primarily the foveola of the eye. They are thought to form due to anterior-posterior forces, tangential forces and weakening in the retinal architecture that result in openings in the macular center.
The International Vitreomacular Traction Study (IVTS) Group formed a classification scheme of vitreomacular traction and macular holes based on OCT findings:
- Vitreomacular adhesion (VMA): No distortion of the foveal contour; size of attachment area between hyaloid and retina defined as focal if </= 1500 microns and broad if >1500 microns
- Vitreomacular traction (VMT): Distortion of foveal contour present or intraretinal structural changes in the absence of a full-thickness macular hole; size of attachment area between hyaloid and retina defined as focal if </= 1500 microns and broad if >1500 microns.
- Full-thickness macular hole (FTMH): Full-thickness defect from the internal limiting membrane to the retinal pigment epithelium. Described 3 factors: 1) Size – horizontal diameter at narrowest point: small (≤ 250 μm), medium (250-400 μm), large (> 400 μm); 2) Cause – primary or secondary; 3) Presence of absence of VMT.
Glaucoma
Glaucoma is a progressive optic neuropathy that is multifactorial and degenerative. It is characterized by the death of retinal ganglion cells (RGCs) and their axons, leading to the characteristic optic disc and retinal nerve fiber layer (RNFL) structural changes and associated vision loss. One of the most effective ways to get information about nerve states is OCT.
The Glaucoma OCT test provides valuable information about ganglion cells: damage to the ganglion cells or their processes leads to thinning across respective layers, which we can measure as the thickness of the ganglion cell complex.
Key things to focus on when working with OCT for glaucoma detection:
- Look for thinning of the pRNFL, particularly in the inferior and superior quadrants, asymmetrical thinning between a patient’s eyes
- Assess the thickness of the ganglion cell-inner plexiform layer, macular RNFL, and the overall ganglion cell complex.
- Monitoring: Seek significant decreases over time in pRNFL thickness (≥5 μm globally, ≥7-8 μm in specific sectors) or in average GCIPL thickness (>4μm).
AI-powered OCT interpretation tools, such as Altris AI, AI for OCT, can further assist clinicians by providing automated calculations of RNFL thinning in the upper and lower hemispheres and the asymmetry levels between them.
Summing up
OCT has revolutionized ophthalmology, bringing a wealth of new details and challenges. The human eye can easily miss subtle abnormalities on complex scans, making accurate interpretation critical. While experience is essential, relying solely on “learning by doing” poses risks.
AI-powered OCT interpretation software bridges this gap, offering a safety net during the learning curve and beyond. AI-powered second opinion on OCT scans enhances diagnostic accuracy, empowers clinicians, and allows them to spend more time for a meaningful connection with patients.
-
Optometry Practice Growth: Business Cases
Altris Inc.
03.10.20248 min readOptometry practice growth: business cases
The client. Dr. William C. Fruchtman’s Optometry Practice, owned and operated by Dr. William C. Fruchtman, O.D., is located in East Rutherford, New Jersey, an inner-ring suburb of New York City. With over 30 years of service to the community, the practice provides comprehensive eye care, including regular eye examinations, contact lenses, and glasses prescriptions.
Dr. William Fruchtman’s practice continually seeks opportunities to add value to its services. He is cultivating his expertise in dry eye disease and macular degeneration, implementing advanced technologies, and using another effective strategy to expand his patient base – communicating with patients in their preferred language. Knowing that clear communication is vital to good care, Dr. William C. Fruchtman’s team includes members who speak Spanish and Polish. As such, their website is available in both Polish and Spanish, a valuable asset considering the area’s substantial Spanish-speaking population (up to 20% of the local demographic).
FDA-cleared AI for OCT analysis
While achieving fluency in every language spoken within your community may not be feasible, consider adapting your website and patient materials to include translations in commonly spoken languages. As Dr. Fruchtman’s experience confirms, even a simple greeting in a patient’s native language can create a bond with patients or, at the very least, prompt a genuine surprised smile.
The problem. To establish expertise in specialized services, Dr. William Fruchtman has been committed to effectively managing dry eye disease and macular degeneration. Not so long ago, the practice implemented Equinox Low-Level Light Therapy (LLLT). This advanced dry eye treatment utilizes LED lights to warm the eyelids gently, promoting meibomian gland function and oil release. With dry eye management addressed, Dr. Fruchtman sought an additional tool to both strengthen his decision-making when managing patients with other pathologies, particularly macular degeneration, and increase his optometry practice growth.
The solution. After researching Altris AI, an Artificial Intelligence platform for OCT scan analysis, Dr. Fruchtman was positive that he wanted to try the platform. Following introductory meetings and a quick onboarding with the Altris team, he started a two-week trial. After personally testing the platform, Dr. Fruchtman decided it was an invaluable addition to his practice.
Integrating Altris AI into the practice has notably enhanced Dr. Fruchtman’s confidence and precision in diagnosing and managing eye care disorders. The practice has also gained a significant competitive advantage, as the platform can routinely perform Glaucoma Risk Analysis on existing OCT scans, offering additional value to patients.
Thanks to the color-coded and labeled OCTs, optometry facilitates patient education and enables practitioners and patients to monitor the progression or treatment results more effectively.
FDA-cleared AI for OCT analysis
How to grow an optometry practice: more cases from optometry owners
Optometrists undergo years of education, training, practice, and continuous learning – understandably, it is hard to see additional time or resources to pursue business education.
Many practitioners experience stress, balancing patient care demands with the realities of running a profitable business. This feeling can intensify when attending countless conferences and webinars highlighting thousands of ways to make business more efficient. While they offer valuable advice, it’s sometimes helpful to remember simple points of how successful optometry practice growth will look: attracting new patients, retaining existing ones, and ensuring a smooth and efficient workflow. These (even though overly simplified) points allow you to focus on the most critical details.
But before diving into ways of optometry practice growth, remember that the first step is a realistic assessment of your current situation.
While you’re likely aware of some issues, feedback from your team and patients can provide insights, and sometimes even immediate solutions, for areas of improvement.
Even though we cannot directly assist in assessing your specific practice, as you know it best, below we offer some key, proven strategies for growing your business.
Optometry practice growth: expanding your patient base
- Dry Eye Specialization
One effective strategy for optometry practice growth is to expand the scope of services to include the diagnosis and management of ocular diseases. For example, dry eye disease (DED) affects ∼344 million people worldwide and over 20 million in the United States alone, yet many remain undiagnosed and untreated. This presents a significant opportunity to care for a large and often underserved patient population. By developing expertise in DED and offering specialized treatments, you can not only attract new patients but also contribute to improving the quality of life for those suffering from this chronic condition.
There are numerous approaches to managing DED effectively. As mentioned, Dr. William C. Fruchtman’s practice utilizes Equinox Low-Level Light Therapy (LLLT).
Dr. Shane Swatts, O.D., owner of Eastern Virginia Eye Associates, employs AI software to enhance DED diagnostics, conduct more comprehensive analyses, and keep detailed patient medical histories. This technology upgrades pre-and post-operative care, saving time without compromising accuracy.
- Aesthetic Optometry
Dr. Janelle Davison identified an opportunity for optometry practice growth by addressing patient needs while generating additional revenue by incorporating aesthetic optometry services into her practice. Within a single quarter, her practice generated $14,000 in revenue from aesthetic product sales alone.
Dr. Davison also collaborates with a licensed aesthetician who operates within the practice on a contract basis, sharing the revenue generated from aesthetic services.
- Glaucoma Management
Dr. James Deom, O.D., M.P.H., an optometrist from Pennsylvania, implemented a successful strategy for optometry practice growth based on attracting glaucoma patients, significantly increasing glaucoma-related revenue. He initiated internal marketing efforts by inquiring about patients’ family history of glaucoma and informing them about the practice’s newest technology for the early detection of vision loss.
Practices specializing in glaucoma management can significantly benefit from incorporating advanced software solutions to complement their existing diagnostic hardware. For instance, integrating Altris AI, AI for OCT, into their OCT analysis workflow enables not only automated screening of 70+ pathologies and biomarkers but includes assessing retinal nerve fiber layer (RNFL) asymmetry for glaucoma risk evaluation.
- Patient-Centered Care
Offering diverse channels for patient interaction can broaden your practice’s reach and improve the patient experience. Dr. Melissa Richard, O.D., sought to provide patients with a preview of frame options before their appointments. To achieve this, she integrated Optify technology into her practice, a solution she discovered during a Vision Source Exchange lecture. This technology creates a virtual showroom where patients can explore and select their preferred frames in advance, streamlining the in-office experience.
Patient education is also key to patient-centered care and personalization, which not only empowers individuals and improves their outcomes but also fosters optometry practice growth. Those who understand their eye health are more likely to adhere to recommendations.
A study demonstrates that 94% desire educational content, but a third don’t receive it.
Providing color-coded OCT reports with pathologies, biomarkers, and pathology progression tracking not only satisfies this need but also elevates your practice above competitors.
Improve efficiency in the optometry office through strategic partnerships & team building
When optometrists consider further career development, they may seek additional support to achieve their goals. Dr. Linda Enciso, O.D., found such support when her practice joined the AEG Vision family in 2019. The transition brought numerous positive changes, boosting patient care and fostering growth opportunities for team members.
Although Dr. Enciso had already been operating her practice for 13 years and had implemented electronic health records (EHR) systems and third-party software to improve patient communication and boost optometry practice growth, her goal was to continue these advancements and expand the scope of practice. Joining AEG Vision allowed her to transition to the training team, access continuing education opportunities to stay informed about advancements in optometry and healthcare, collaborate with other healthcare providers and cross-functional teams to enhance comprehensive patient care.
While the phrase “team building” might evoke images of complicated activities and extensive effort, fostering a strong team can be achieved through simple, engaging initiatives. Consider the inspiring example of Dr. Jonathan Cargo, O.D.
Dr. Cargo recognizes the value of personal development through reading but finds it challenging to share his insights with his team effectively. Inspired by his wife’s long-standing book club, he initiated an office book club to encourage team connection and shared learning to improve efficiency in the optometry office.
The book club operates with team members suggesting relevant titles and collectively reading chapters over a month, dedicating time during team meetings for discussions. Dr. Cargo highlights the recent success of reading “Crucial Conversations,” a selection prompted by team members’ desire to deepen their communication skills, particularly in navigating challenging discussions with colleagues, patients, and even family members. The shared reading experience gave a better understanding of effective communication strategies and empowered the team to navigate difficult conversations.
Summing up
When regarding optometry practice growth, consider the time, effort, and resources you are prepared to invest. To expand your patient base, explore the addition of new services.
FDA-cleared AI for OCT analysis
To optimize costs and efficiency and gain a competitive edge, investigate the possibility of implementing AI in your practice – it can be a second-opinion tool, or you can read here how practitioners use it for marketing, creating educational materials, and more. To encourage staff retention and nurture a positive work environment, prioritize team-building activities; even seemingly simple initiatives can produce significant benefits.
-
Optometry Trends in Action: 12 Real-World Success Stories
Maria Znamenska
17.09.20248 min readOptometry Trends in Action: 12 Real-World Success Stories
Optometry trends explained: showcasing real-world optometry practice owners who are adapting to the shift in patient needs, successfully implementing solutions to automate routine and laborious tasks, using AI to combat staff shortages, creating their own brand mascots, and more.
FDA-cleared AI for OCT analysis
Optometry trends for the patient journey: digital communication
Online shopping, global deliveries, and instant brand replies through messengers have dramatically shifted client expectations and behaviors. The ‘convenience economy’ isn’t slowing down, pushing businesses to adopt technology for more streamlined consumer experiences.
What does this mean for your practice? Your patients now expect fast and efficient communication across all touchpoints – from online scheduling to contactless payments. Transforming your practice to meet these demands ensures satisfied patients and contributes to long-term success, as any optometry practice thrives on the individual experiences of the patients it provides.
46% of optometrists reported that patient expectations have risen since the pandemic.
Practices can optimize their workflows in various ways, but generally, the goal is to automate routine administrative tasks, free up staff, and reduce patient waiting time. Digital safety forms and document management systems eliminate physical paperwork, while online proofing and approval systems speed up document processing.
Dr. Justin Bazan, owner and optometrist at Park Slope Eye, New York, has taken this even further by eliminating phone calls at his office entirely and is pleased with the results. This solution was based on several months of analyzing data related to phone calls, including time spent on calls and the frequency of missed calls. The team recognized that while the staff could simultaneously chat with multiple patients, they could only handle one phone call at a time.
Chad Fleming, OD, Owner and OD at Wichita Optometry, Kansas, also identified the need for an enhanced digital presence to prioritize patient convenience. His practice faced the challenge of managing a high volume of phone calls and text messages, requiring either additional staff hiring without an immediate increase in revenue or a strategic reallocation of existing personnel.
Dr. Fleming optimized the patient experience by setting up automated checkouts at some of his practice locations. This approach enabled him to reassign three front desk employees to the digital communications team. While the transition required patient education to familiarize them with the virtual check-in process on iPads, it did not result in patient attrition.
Brianna Rhue, OD, Owner and Optometrist of West Broward Eyecare Associates, Florida, agrees that the traditional approach of answering calls and checking emails once a day differs from today’s patient expectations. She advocates step-by-step optimizations throughout the patient journey to eliminate unnecessary wait times and increase productivity.
Upgrading to a more advanced EHR system is one of the significant opportunities to streamline practice operations, save practitioners time, money, and stress, and align with optometry industry trends. Unfortunately, once hailed as revolutionary, some widely adopted EHR solutions are now criticized for their burdensome workflows and counterintuitive interfaces. This has led some practitioners to describe their interaction with systems as “death by a thousand clicks.”
By leveraging up-to-date EHR features like customizable patient encounter templates, integrated imaging and diagnostic tools, and patient outcome tracking, eye care professionals can shift their focus from paperwork to patient care.
Another of optometry trends gaining momentum among optometry practice owners is offering flexible payment options. This reflects not only the growing demand for convenience but also the financial constraints of patients navigating the current economy that is heading to a recession.
Dr. Rhue encourages practices to adopt mobile payment solutions that enable patients to pay electronically using platforms like Apple Pay, Venmo, or PayPal at the point of service. For balances due after the visit, the ability to send secure payment links via text message can greatly enhance the collection process.
Furthermore, providing patient financing options empowers patients to choose how and when they pay. This offers additional convenience for both parties and eliminates friction by allowing patients to spread the cost of their care over time rather than requiring full payment upfront.
If you are still determining which technologies of these optometry industry trends your patients will be eager to adopt, consider the approach taken by Scott Jens, OD, the owner of Isthmus Eye Care, Wisconsin. Dr. Jens has successfully implemented post-examination surveys to gather patient feedback. This strategy serves a dual purpose: demonstrating your commitment to patient satisfaction and gaining valuable insights into which technological advancements would most benefit your practice.
Optometry trends in the exam room: tech-driven precision and patient education
Optometry relies heavily on technology, and investing in hardware upgrades is a significant financial commitment. However, if your hardware needs are met, but you still want to be at the forefront of technological advancements, consider specialized software and platforms to extend the possibilities of your existing devices.
Dr. Maria Sampalis, OD, the owner of Sampalis Eye Care, Rhode Island, utilizes two such programs in her practice. To support her specialization in dry eye management, she employs CSI Dry Eye. Additionally, she uses Altris AI, an AI-powered platform for OCT scan analysis, to provide a second opinion and enhance diagnostic accuracy.
Dr. Sampalis finds that the Dry Eye software allows her and her staff to analyze symptoms and images comprehensively, improving patient care, time savings, and increasing diagnostic precision. See how OCT AI works here.
Her patients also appreciate Altris AI, which analyzes OCT scans for over 70 pathologies and biomarkers while also calculating the risk of developing glaucoma.
Working with specialized software solutions improves diagnostic accuracy and aids in patient education. Visual representations of their conditions, facilitated by these technologies, empower patients with a clearer understanding, leading to increased treatment compliance.

Eye Place, an optometry center in Columbia, also leverages Altris AI, among other cutting-edge technologies. They capture images using the Topcon Maestro2 OCT and use Image Net6 software to export DICOM files to the Altris AI platform.
Beyond AI-powered OCT analysis, Eye Place utilizes state-of-the-art diagnostic tools, such as 3D OCT equipment, to screen for serious conditions, including glaucoma, diabetes, and macular degeneration. Furthermore, they work with AdaptDX Pro, a technology capable of detecting macular degeneration earlier than traditional methods.
Another case of optimizing and enhancing the exam process is West Broward Eyecare Associates. They implemented Optify, a smart building solution offering full fiber connectivity. Patients can pre-select frames in the online optical store before their visit, streamlining the in-office experience. Additionally, the practice utilizes Dr. Contact Lens, a platform for convenient ordering, reordering, and prescription management for contact lens wearers, reducing paper waste.
There are also advancements in AI transcription technology that are poised to ease clinical documentation and automate a traditionally laborious task.
The adoption of AI in clinical documentation has been shown to reduce the time doctors spend on charting by approximately 2 hours per day.
AI exam transcription is still in the process, and the existing possibilities are not yet flawless—struggling with patient responses like “mm-hm” and “uh-huh”—the technology is evolving, promising greater efficiency and accuracy in the future. For example, one such program starts the transcription process of the exam by confirming patient consent and a click of the record button by the optometrist. Then, AI captures, structures, and summarizes information in real-time, filtering for relevant details to generate documentation for each patient appointment.
Optometry trends for competitive advantage: using AI in Marketing and Decision-making
Some practice owners may still believe their patient demographics do not necessitate an expanded online presence, particularly when considering elders. But you should be different from your competitors.
The reality is that today’s patients, regardless of age, are increasingly turning to the Internet for information and services. While word-of-mouth referrals remain valuable, a solid online presence is essential for practice growth and visibility in today’s competitive landscape.
Twin Forks Optometry and Vision Therapy in New York reports that their most effective marketing strategy involves a monthly-to-quarterly newsletter distributed to existing patients. This newsletter highlights practice updates, recent vision therapy graduates, new podcast episodes, and seasonal information. They’ve also observed that educational posts generate significant engagement and have even led to new patient visits.
Voice Search Optimization (VSO) is emerging as one of the new trends in optometry that has the potential to benefit practices significantly. Dr. Brianna Rhue, OD, co-owner of West Broward Eyecare Associates in Florida, asserts that a search engine optimized (SEO) website alone will soon be insufficient for patients to discover your practice online easily, especially in highly competitive locations.
Contrary to popular belief, it’s not just the tech-savvy individuals who rely on voice assistants. This technology is predominantly used by older individuals who haven’t mastered typing or face difficulties with it.
However, while the benefits of digital communication are undeniable, it’s crucial to acknowledge that it often adds up yet another layer of responsibility to already overburdened teams. This is why generative AI tools like ChatGPT and Gemini are gaining popularity among optometrists, offering solutions to this and other challenges.
For example, Dr. Ryan Cazares, the owner and founder of Scott Eye Care in Louisiana, utilizes ChatGPT to generate social media and educational content for his practice. He brainstorms with AI content ideas, creates visuals for social media and marketing campaigns, and has even developed a unique mascot (Dr. Seymour) that engages his audience.
The practitioner also uses AI to generate personalized educational materials for their patients. Traditionally, his practice relied on generic Optometric Association pamphlets, but now, it has transitioned to simple one-page educational sheets tailored to individual patient needs.
Dr. Haley Perry, owner of Elite Eye Care, New York, provides another example of AI’s potential in practice management. Her goal for this year was to increase patient volume without expanding her staff, and ChatGPT played a pivotal role in achieving this objective.
Faced with the decision between two vendors for new exam room equipment, she used AI to analyze each vendor’s pricing and financing options, weigh the pros and cons of the equipment in relation to her goals, and forecast the return on investment (ROI) for each option. This analysis enabled her to select the most suitable vendor and estimate the timeframe for recouping her investment.
Dr. Perry also leverages AI to analyze patient feedback, demographic data, and treatment outcome statistics to ensure equipment investments align with patient needs. For instance, if data reveals a high prevalence of conditions like glaucoma, AI can help justify investing in advanced glaucoma screening tools.
FDA-cleared AI for OCT analysis
Summing up
The optometry landscape is evolving, driven by raised patient expectations for convenience and efficiency. Practices adapt to these changes by embracing emerging optometry trends to achieve more precise diagnostics, streamline patient journeys, enhance the exam room experience, and build trust and connection. Much of this technology is AI-based, with even more advancements on the horizon. So, optometrists implementing these solutions today are poised to secure a significant competitive advantage.
-
How we build Ethical AI at Altris AI
Andrey Kuropyatnyk
03.09.202413 min readHow we build Ethical AI at Altris AI
As the co-owner of the AI HealthTech startup, I get many questions regarding biases and the security of our AI algorithm. After all, Altris AI works directly with patients’ data, which is why these questions are inevitable and even expected. So, I decided to share our approach to building Altris AI as an ethical AI system.
From the very first moments of the company’s creation, I knew that AI and healthcare were two topics that had to be handled very carefully. That is why we ensured that every aspect of the AI platform creation aligned with modern security and ethics guidelines.
It’s like building a house: you need to take care of the foundation before getting to the walls, roof, and decor. Without it, everything will fall sooner or later. Ethical principles of AI are this foundation.
The following aspects of Ethical AI were the most important for us: machine training ethics, machine accuracy ethics, patient-related ethics, eye care specialists-related ethics, usefulness, usability, and efficiency.
FDA-cleared AI for OCT analysis
1. Machine Training Ethics
To create an accurate algorithm capable of analyzing OCT scans, we needed to train it for years. When it comes to machine training, we speak about data for this training. There are 2 major aspects of machine training ethics that need to be discussed: data ownership and data protection.
Data ownership/Data privacy indicates authority to control, process, or access data. By default, all patients’ data belongs exclusively to patients; no one owns it and sells it to a third party. For Altris AI machine training, all the data was obtained from patients directly who voluntarily agreed to share it and signed relevant documents.
More than that, no client’s data, under any circumstances, is used to train the Altris AI.

Data protection
- GDPR
Currently, there are the following regulations to protect the confidentiality of patients’ data. The European Union (EU) has legislatures of General Data Protection Regulation (GDPR), Cybersecurity Directive, and Medical Devices Regulation.
- HIPAA
In the US, the Health Insurance Portability and Accountability Act (HIPAA) is suggested as a counterpart for European legislation to cover wider confidentiality issues in medical data.
At Altris AI, we obtained EU certification and ensured that all data is GDPR and HIPAA-compliant. This also applies to all the patients’ data we receive.
- European Union Artificial Intelligence Act
Provider obligations
As a provider of a high-risk AI system, we comply with the obligations listed under Article 16.
High-risk obligations
Under Article 6, high-risk obligations apply to systems that are considered a ‘safety component’ of the kind listed in Annex I Section A, and to systems that are considered a ‘High-risk AI system’ under Annex III.
At Altris AI we followed these obligations:
- Established and implemented risk management processes according to Article 9.
- Used high-quality training, validation, and testing data according to Article 10.
- Established documentation and design logging features according to Article 11 and Article 12.
- Ensured an appropriate level of transparency and provided information to users according to Article 13.
- Ensured human oversight measures are built into the system and/or implemented by users according to Article 14.
- Ensured robustness, accuracy, and cybersecurity according to Article 15.
- Set up a quality management system according to Article 17.
Transparency Obligations
At Altris AI we also followed the transparency obligations under Article 50:
- The AI system, the provider or the user must inform any person exposed to the system in a timely, clear manner when interacting with an AI system, unless obvious from context.
- Where appropriate and relevant include information on which functions are AI-enabled, if there is human oversight, who is responsible for decision-making, and what the rights to object and seek redress are.
2. Machine Accuracy Ethics.
Data transparency.
Where transparency in medical AI should be sought?
Transparency in Data Training:
1. What data was the model trained on? Including population characteristics and demographics.
The model’s proprietary training data set was collected from patients from several clinics who consented to share their data anonymously for research purposes. The dataset includes diverse and extensive annotated data from various OCT scanners, encompassing a range of biomarkers and diseases. It does not specifically target or label demographic information, and no population or demographic information was collected.
2. How was the model trained? Including parameterization and tuning performed.
The training process for the deep learning model involves several steps:- Data Annotation: Medical experts annotated the data, creating the ground truth for biomarker segmentation.
- Data Preprocessing: The data is augmented using unsupervised techniques (e.g., albumentations library) to increase diversity during training.
- Model Architecture: The model’s architecture is based on the UNet model with ResNet backbones, incorporating additional training techniques specifically engineered for OCT images.
- Training Process: The model is trained using supervised learning techniques to predict the output biomarker segmentation mask and diagnosis label, employing backpropagation and gradient descent to minimize the loss function.
- Parameterization: The model has millions of parameters (weights) adjusted during training. Hyperparameters such as learning rate, batch size, and the number of layers are tuned to optimize performance.
- Tuning: Hyperparameter tuning is performed using techniques like grid search, random search, or Bayesian optimization to find the optimal set of parameters that improve the model’s performance on validation data.
3. How has the model been trained to avoid discrimination?
The model training uses a wide variety of data to ensure exposure to different perspectives, reducing the likelihood of reinforcing a single viewpoint. No data related to race, gender identification, or other sensitive attributes is used at any stage of the model’s lifecycle (training, validation, inference). The model solely requires OCT images without additional markers or information.4. How generalizable is the model? Including what validation has been performed and how do you get comfortable that it generalizes well.
- Validation Methods: The model is validated using a variety of images that were not seen during training.
- Performance Metrics: Metrics like Dice and F1 score are used to evaluate the model’s performance.
- Cross-Domain Testing: The model is tested on images from different OCT scanners and time frames to ensure it can generalize well.
- User Feedback: Real-world usage and feedback help identify areas where the model may not generalize well, allowing for continuous improvement.
5. How explainable is the model? Including what explainability testing has been done, if any.
Explainability Techniques: Techniques like SHAP (SHapley Additive exPlanations), GradCAM, and activation visualization are used to understand which parts of the input images the model focuses on when making predictions.
Medical Expert Testing: Regular testing and analysis are conducted to ensure that the model’s detections make sense to medical experts and that the model’s decisions align with logical and reasonable patterns.
Any AI system is opaque (unintelligible) for two reasons:
- Innate complexity of the system itself.
- Intentional proprietary design for the sake of secrecy and proprietary interests.
Biases. In most instances, an AI tool that gives a wrong decision usually reflects biases inherent in the training data. Biases might be racial, ethnic, genetic, regional, or gender-based.
There should not be any bias related to race and ethnicity because there is no evidence that biomarkers and pathologies manifest themselves differently in patients of different races and ethnicities. Altris AI uses sufficiently diverse gender and age-related data to provide accurate results for OCT analysis.
3. Patient-related ethics.
Patient-related ethics in AI are based on the rights of beneficence, nonmaleficence (safety), autonomy, and justice. Patients exercise their rights either explicitly through informed consent or implicitly through norms of confidentiality or regulatory protections.
Informed Consent.
Informed consent is based on the principle of autonomy. It could authorize the partial or complete role of algorithms in health care services and detail the process of reaching diagnostic or therapeutic decisions by machines. Clinicians should explain the details of these processes to their patients. Patients should have the choice to opt in or out of allowing their data to be handled, processed, and shared.
As these rights can be enabled by eye care professionals, they remain on the side of eye care professionals in our case. However, eye care professionals who use Altris AI not only inform patients about using AI for OCT scan analysis but also use the system to educate patients with the help of color coding.

Confidentiality.
Patients’ confidentiality is a legal obligation and a code of conduct. Confidentiality involves the responsibility of those entrusted to handle and protect patient’s data.
All the data that is used inside the Altris AI platform is anonymized and tokenized, and only eye care professionals who work with patients see any personal information. For the Altris AI team, this data is viewed as a programming code.
4. Eye care specialist-related ethics.
AI systems, like Altris AI, are unable to work 100% autonomously, and therefore, eye care specialists who use them should also make ethical decisions when working with AI.
Overreliance on AI. One of the important aspects of physician-related ethics is overreliance on AI during diagnostic decisions. We never cease to repeat that Altris AI is not a diagnostic tool in any sense; it is a decision-making support tool. The final decision will always be made by an eye care professional. It is an eye care professional who must take into consideration the patient’s clinical history, the results of other diagnostic procedures, lab test results, concomitant diseases, and conclusions from the dialogue with the patient to make the final decision.
Substitution of Doctors’ Role. Considering the information mentioned above, it is important to clarify the aspect of substituting eye care specialists. It should always be kept in mind that the aim of adopting AI is to augment and assist doctors, not to replace them.
Empathy. Empathetic skills and knowledge need to be further incorporated into medical education and training programs. AI performing some tasks offers space for doctors to utilize empathy in medical education and training.
FDA-cleared AI for OCT analysis
5. Usefulness, Usability, and Efficacy.
According to the Coalition for Health AI (CHAI) checklist, AI in healthcare must be, first of all, useful, usable, and efficient.
To be useful, an AI solution must provide a specific benefit to patients and/or healthcare delivery and prove to be not only valid and reliable but also usable and effective. The benefit of an AI solution can be measured based on its effectiveness in achieving intended outcomes and its impact on overall health resulting from both intended and potentially unintended uses. An assessment of benefits should consider the balance between positive effects and adverse effects or risks.
In the case of Altris AI, its usefulness is proved by the clients’ testimonials we receive regularly.
Relatedly, an effective AI solution can be shown to achieve the intended improvement in health compared to existing standards of care, or it can improve existing workflows and processes.
With Altris AI, we make patient screening and triage faster and more effective. We also significantly improve the detection of early pathologies, such as early glaucoma, which are often invisible to the human eye.
Usability presupposes that the AI tool must be easy for healthcare practitioners. Altris AI is actively used by more than 500 eye care businesses worldwide, proving its usability. Moreover, we constantly collect feedback from users and improve the platform’s UI/UX.
Conclusion
Recently Posted
-
AI for Decision Support with OCT: “Altris AI Gave Me More Certainty in My Clinical Decisions”
Maria Martynova
2 minutesAI for Decision Support with OCT: An Interview with Clara Pereira, Optometrist from Franco Oculista
About Franco Oculista Optometry in Portugal.
Franco Oculista is the optometry center with a 70-year-old history: its roots date back to the mid-1950s in Luanda, where it was founded by Gonçalo Viana Franco. Having left behind a career in pharmacy, Gonçalo pursued his entrepreneurial vision by opening an optician’s bearing his name in the heart of the Angolan capital. Driven by a thirst for knowledge and a deep sense of dedication, he turned his dream into reality. With a commitment to professionalism and a forward-thinking approach, he integrated the most innovative technologies available at the time. This blend of passion, expertise, and innovation established Franco Oculista as a benchmark for quality and excellence in the field. In 1970s, the family returned to Portugal and opened the new FRANCO OCULISTA space on Avenida da Liberdade.
How do Franco Oculista describe their mission?
“Through individualized and segmented service, we seek to respond to the needs of each client. We combine our knowledge with the most sophisticated technical equipment and choose quality and reliable brands. We prioritize the evolution of our services and, for this reason, we work daily to satisfy and retain our customers with the utmost professionalism.”
Clara Pereira is one of the optometrists at Franco Oculista and has been an optometrist for nearly two decades. Based in a private clinic in Portugal, she brings years of experience and calm confidence to her consultations. We talked with her to learn how her clinical practice has evolved, particularly since integrating OCT and, more recently, Altris AI – AI for Decision Support with OCT.
Altris AI: Clara, can you tell us a bit about your daily work?
Clara: “Of course. I’ve been working as an optometrist for 19 years now. My practice is quite comprehensive—I assess refractive status, binocular vision, check the anterior segment with a slit lamp, measure intraocular pressure, and always examine the fundus.
Clara: “In Portugal, we face limitations. We’re not allowed to prescribe medication or perform cycloplegia, so imaging becomes crucial. I rely heavily on fundus photography and OCT to guide referrals and detect early pathology.”
Altris AI: How central is OCT diagnostics to your workflow?
Clara: “OCT is substantial. I perform an OCT exam on nearly every patient, on average, eight OCT exams per day. It’s an essential part of how I gather information. With just one scan, I can learn so much about eye health.”Altris AI: What kind of conditions do you encounter most frequently?
Clara: “The most common diagnosis is epiretinal membrane—fibrosis. But I also manage patients with macular degeneration and other retinal pathologies. Having the right tools is key.”Altris AI: And what OCT features do you use the most?
Clara: “I regularly use the Retina, Glaucoma, and Macula maps. But if I had to choose one, the Retina Map gives me the most complete picture. It’s become my go-to.”Altris AI: You’ve recently started using Altris AI. What has that experience been like?
Clara: “At first, I didn’t know much about it. But when Optometron introduced Altris AI to me—a company I trust—I didn’t hesitate. And I’m glad I didn’t. From the beginning, it felt like a natural extension of my clinical reasoning.Clara: “Altris AI gives me an extra layer of certainty. It helps me extract more from the OCT images. I usually interpret the scan myself first, and then I run it through the platform. That way, I validate my thinking while also learning something new.”
Altris AI: Have any standout cases where Altris AI made a difference?
Clara: “Yes. I’ve had a few. One was a case of advanced macular degeneration, in which the AI visualization really helped me explain the condition to the patient. Another was using anterior segment maps for fitting scleral lenses—Altris was incredibly useful there, too. I do a lot of specialty lens fittings, so that was a big advantage.”
Altris AI: Would you recommend Altris AI to your colleagues?
Clara: “I would recommend Altris AI to my colleagues. For me, it’s about more than just the diagnosis. It’s about feeling confident that I’m seeing everything clearly and giving my patients the best care possible. Altris AI helps me do exactly that.”
Why This Matters: Altris AI in Real Practice
Clara’s story reflects the real value of AI in optometry—not as a replacement for clinical judgment, but as a powerful companion. With every OCT scan, she strengthens her expertise, improves diagnostic accuracy, and gives her patients the reassurance they deserve.
Whether identifying early signs of fibrosis, supporting complex scleral lens fittings, or acting as a second opinion, Altris AI seamlessly fits into the modern optometrist’s workflow, making every scan more meaningful.
AI for Decision Support with OCT: Transforming Retinal Diagnostics
Artificial Intelligence (AI) is revolutionizing the field of ophthalmology, particularly through its integration with Optical Coherence Tomography (OCT). OCT is a non-invasive imaging technique that captures high-resolution cross-sectional images of the retina, enabling early detection and monitoring of various ocular conditions. However, interpreting these scans requires time, expertise, and consistency—factors that AI-based decision support systems are uniquely positioned to enhance.
Altris AI (AI for OCT decision support platform) analyzes thousands of data points across B-scans, automatically detecting retinal pathologies, quantifying biomarkers, and identifying patterns that may be subtle or overlooked by the human eye. By providing objective, standardized assessments, Altris AI reduces diagnostic variability and improves clinical accuracy, especially in busy or high-volume practices.
For optometrists and ophthalmologists, AI acts as a second opinion, flagging early signs of diseases such as age-related macular degeneration (AMD), diabetic retinopathy, and glaucoma. It streamlines workflows by highlighting areas of concern, prioritizing cases that require urgent attention, and offering visual explanations that are easy to communicate to patients.
Moreover, Altris AI enableS longitudinal tracking of pathology progression. By comparing OCT scans over time ( even from various OCT devices), clinicians can monitor subtle changes in drusen volume, retinal thickness, supporting timely clinical decisions and tailored treatment strategies. The integration of AI into OCT interpretation not only enhances diagnostic confidence but also supports evidence-based care, early intervention, and improved patient outcomes. As AI continues to evolve, it will play a vital role in advancing precision medicine in ophthalmology, empowering eye care professionals with tools that are fast, reliable, and scalable.
In essence, AI for OCT decision support is not replacing clinical expertise; it is augmenting it, elevating the standard of care through speed, accuracy, and actionable insights.
-
Best AI for OCT: 10 Essential Features Your Platform Must Have
Maria Martynova
8 min.Best AI for OCT: 10 Essential Features Your Platform Must Have
So you’ve decided to trial AI for OCT analysis and wondering how to choose among all the available platforms. To save you some time, we’ve collected 10 most essential criteria according to which you can assess all existing AI platforms. Using this criteria you will be able to make an informed and rational choice.
As an ophthalmologist, I am interested in finding innovative and modern approaches that could help me to enhance the workflow and improve patient outcome as a result.Analyzing various platforms, I realized that these 10 criteria are crucial for the right choice.
1. Regulatory Compliance and Clinical Validation
In healthcare, safety is always first. Regulatory approval and clinical validation are essential for AI-powered platforms for OCT scan analysis.
The best AI OCT platforms should meet regulatory standards set by authorities such as the FDA, HIPAA, CE, and ISO.
Adhering to regulatory guidelines enhances credibility and fosters trust among healthcare professionals. Check if the AI for OCT analysis tool has all these certificates in place and if they are valid.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
2.Wide range of biomarkers and pathologies detected
Some AI for OCT platforms concentrate on certain pathologies, like Age-Related Macular Degeneration (AMD) or Diabetic Retinopathy, because of the prevalence of these conditions among the population. It mostly means that eye care specialists must know in advance that they are dealing with the AMD patient to find the proof of AMD on the OCT.
The best AI for OCT tools should have a wide variety of biomarkers and pathologies, including rare ones that cannot be seen daily in clinical practice, such as central retinal vein and artery occlusions, vitelliform dystrophy, macular telangiectasia and others. Altris AI, the leader of OCT for AI analysis, detects 74 biomarkers and pathologies as of today.
3.Cloud-Based Data Management and Accessibility
To ensure seamless integration into clinical workflows, the AI OCT platform should offer cloud-based data management and accessibility. Cloud storage allows for easy retrieval of patient records, remote consultations, and multi-location access. Secure cloud computing also enhances collaboration between ophthalmologists, optometrists, and researchers by enabling data sharing while maintaining compliance with data privacy regulations such as HIPAA and GDPR.
Many clinics have strict policies regarding patient data storage as well: it is crucial that the data is stored on the servers in the region of operation. If the clinic is in EU, the data should be stored in the EU.
4.Real-world usage by eye care specialists
When choosing the best AI for OCT analysis, real-world usage by eye care specialists is the most critical factor. Advanced algorithms and high accuracy metrics mean little if the AI is not seamlessly integrated into clinical workflows and actively used by optometrists and ophthalmologists. There are thousands of research models available, but when it comes to the implementation, most of them are not available to ECPs.
Eye care professionals are not IT specialists. They require AI that is intuitive, fast, and reliable. If a system disrupts their workflow, generates excessive false alerts, or lacks clear explanations for its findings, adoption rates will be low—even if the technology itself is powerful. The best AI solutions are those that specialists trust and rely on daily to enhance diagnostic accuracy, streamline patient management, and support decision-making.
Moreover, real usage generates valuable feedback that continuously improves the AI. Systems actively used in clinical settings undergo rapid validation, refinement, and adaptation to diverse patient populations. This real-world data is far more meaningful than isolated test results in controlled environments.
5. Customizable Reporting and Visualization Tools
Reports are the result of the whole AI for OCT scan analysis that is why customizable and comprehensive reports are a must.
A high-quality AI OCT platform must offer customizable reporting and visualization tools. Clinicians should be able to adjust parameters, select specific data points, and generate detailed reports tailored to individual patient needs.
Heatmaps, 3D reconstructions, and trend analysis graphs should be available to help visualize disease progression. These tools improve the interpretability of AI-generated insights and facilitate patient education.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
6.AI for Early Glaucoma Detection
Glaucoma is a leading cause of irreversible blindness, and since OCT is widely used to assess the retinal nerve fiber layer (RNFL), Ganglion Cell Complex ( GCC), optic nerve head (ONH), AI can significantly enhance early detection and risk assessment.
Therefore, the best AI for OCT analysis tools have an AI for early glaucoma detection module available to assess the risk of glaucoma especially at the early stage. Moreover, tracking the progression of glaucoma with the help of AI should also be available for eye care specialists.
Clear and bright notifications about glaucoma risk are also vital for making AI glaucoma modules easy to use. AI can provide proactive insights that enable early intervention and personalized treatment plans
7.User – Friendly Interface and Intuitive Workflow Integration
A well-designed AI OCT platform should feature a user-friendly interface that integrates seamlessly into existing clinical workflows.
It means that even non-tech-savvy eye care specialists should be able to navigate it effortlessly.
The interface should be intuitive, reducing the learning curve for healthcare providers. Features such as automated scan interpretation, voice command functionality, and guided step-by-step analysis can enhance usability and efficiency.
8.Integration with Electronic Health Records (EHRs)
For a seamless clinical experience, the AI OCT platform should integrate with existing electronic health record (EHR) systems. Automated data synchronization between AI analysis and patient records enhances workflow efficiency and reduces administrative burden. This feature enables real-time updates, streamlined documentation, and easy access to past diagnostic reports.
9. Universal AI solutions compatible with all OCT devices
Uf you want to use AI to analyze OCT, this AI should be trained on data received from various OCT devices and therefore should be applicable with various OCT devices. A vendor-neutral AI tool for OCT analysis provides unmatched advantages over proprietary solutions tied to specific hardware. By working seamlessly with multiple OCT devices, it eliminates the need for costly equipment upgrades and ensures broader accessibility across clinics and hospitals.
This approach also fosters greater innovation, allowing AI models to continuously improve based on diverse datasets rather than being limited to a single manufacturer’s ecosystem. Vendor-neutral solutions integrate effortlessly into existing workflows, reducing training time and boosting efficiency. Clinicians benefit from unbiased, adaptable technology that prioritizes patient outcomes rather than locking users into restrictive ecosystems.
10. Cost-Effectiveness and Accessibility
To maximize its impact, an AI-powered OCT platform should be cost-effective and accessible to a wide range of healthcare providers. Affordable pricing models, including subscription-based or pay-per-use plans, can make AI technology available to smaller clinics and developing regions. Accessibility ensures that AI-driven OCT analysis benefits as many patients as possible, improving global eye health outcomes.
FDA-cleared AI for OCT analysis
Trial AI for OCT or learn more about it
Conclusion
What is the best AI for OCT scan analysis? The best AI for OCT must be a comprehensive, intelligent, and adaptable platform that enhances diagnostic accuracy, streamlines clinical workflows, and supports proactive eye care. Key features such as high-accuracy automated analysis, multi-modal imaging integration, real-time decision support, cloud-based data management, interoperability, and explainable AI decision-making are crucial for an effective OCT AI system. By incorporating these attributes, AI-driven OCT platforms can revolutionize ophthalmology, enabling early disease detection, personalized treatment planning, and improved patient outcomes. As AI technology continues to advance, its integration with OCT will play an increasingly vital role in shaping the future of eye care.
-
Future of Ophthalmology: 2025 Top Trends
Maria Znamenska
13.03.202512 min readFuture of Ophthalmology: 2025 Top Trends
In a recent survey conducted by our team, we asked eye care specialists to identify the most transformative trends in ophthalmology by 2025. The results highlighted several key areas, with artificial intelligence (AI) emerging as the clear frontrunner, cited by 78% of respondents.
However, the survey also underscored the significant impact of optogenetics, novel AMD/GA therapies, and the continuing evolution of anti-VEGF treatments. This article will explore the practical implications of these advancements, providing an overview of how they are poised to reshape diagnosis, treatment, research, and, ultimately, patient outcomes in ophthalmology.
In this article, we will also discuss Oculomics, a very promising field that is gaining momentum.
FDA-cleared AI for OCT analysis
Top AI Technology for Detecting Eye-related Health Risks 2025
Building upon the survey’s findings, we begin with the most prevalent trend: top AI technology for detecting eye-related health risks in 2025
AI in Clinical Eye Care Practice
With the increasing prevalence of conditions like diabetic retinopathy and age-related macular degeneration, there is a growing need for efficient and accurate screening tools. And AI is already valuable for eye-care screening: algorithms can analyze retinal images and OCT scans to identify signs of these diseases, enabling early detection and timely intervention.
AI-powered screening tools can also help identify rare inherited retinal dystrophies, such as Vitelliform dystrophy and Macular telangiectasia type 2. These conditions can be challenging to diagnose, but AI algorithms can analyze retinal images to detect subtle signs that human observers may miss.
AI also starts to play a crucial role in glaucoma management. Early detection of glaucoma demands exceptional precision, as the early signs are often subtle and difficult to detect. Another significant challenge in glaucoma screening is the high rate of false positive referrals, which can lead to unnecessary appointments in secondary care and cause anxiety for patients, yet delayed or missed detection of glaucoma results in irreversible vision loss for millions of people worldwide. So, automated AI-powered glaucoma analysis can offer transformative potential to improve patient outcomes.
One example of promising AI technology is Altris AI, artificial intelligence for OCT scan analysis, which has introduced its Advanced Optic Disc (OD) Analysis that provides a comprehensive picture of the optic disc’s structural damage, allowing detailed glaucoma assessment for treatment choice and monitoring.
This OD module evaluates optic disc parameters using OCT, providing personalized assessments by accounting for individual disc sizes and angle of rim absence. Such a tailored approach eliminates reliance on normative databases, making evaluations more accurate and patient-specific.
Furthermore, it enables cross-evaluation across different OCT systems, allowing practitioners to analyze macula and optic disc pathology, even when data originates from multiple OCT devices. Key parameters evaluated by Altris AI’s Optic Disc Analysis include disc area, cup area, cup volume, minimal and maximum cup depth, cup/disc area ratio, rim absence angle, and disc damage likelihood scale (DDLS).
AI for Clinical Trials and Research
AI is revolutionizing clinical trials and research in ophthalmology. One such key application of AI is biomarker discovery and analysis. Algorithms can analyze large datasets of medical images, such as OCT scans, to identify and quantify biomarkers for various eye diseases. These biomarkers can be used to assess disease progression, monitor treatment response, and predict clinical outcomes.
AI is also being used to improve the efficiency and effectiveness of clinical trials. By automating the process of identifying eligible patients for clinical trials, AI can help researchers recruit participants more quickly and ensure that trials include appropriate patient populations, accelerating the development of new treatments.
Algorithms can analyze real-world data (RWD) collected from electronic health records and other sources to generate real-world evidence (RWE). RWE provides valuable insights into disease progression, treatment patterns, and long-term outcomes in everyday clinical settings, complementing the findings of traditional randomized controlled trials.
Oculomics
Integrating digitized big data and computational power in multimodal imaging techniques has presented a unique opportunity to characterize macroscopic and microscopic ophthalmic features associated with health and disease, a field known as oculomics. To date, early detection of dementia and prognostic evaluation of cerebrovascular disease based on oculomics has been realized. Exploiting ophthalmic imaging in this way provides insights beyond traditional ocular observations.
For example, the NeurEYE research program, led by the University of Edinburgh, is using AI to analyze millions of anonymized eye scans to identify biomarkers for Alzheimer’s disease and other neurodegenerative conditions. This research can potentially revolutionize early detection and intervention for these devastating diseases.
Another effort spearheaded by researchers from Penn Medicine, Penn Engineering is exploring the use of AI to analyze retinal images for biomarkers indicative of cardiovascular risk. AI systems are being trained on fundus photography to detect crucial indicators, such as elevated HbA1c levels, a hallmark of high blood sugar, and a significant risk factor for both diabetes and cardiovascular diseases.
AI analysis of retinal characteristics, such as retinal thinning, vascularity reduction, corneal nerve fiber damage, and eye movement, has shown promise in predicting Neurodegenerative diseases. Specifically, decreases in retinal vascular fractal dimension and vascular density have been identified as potential biomarkers for early cognitive impairment, while reductions in the retinal arteriole-to-venular ratio correlate with later stages.
Moving from AI, we now turn to another significant trend identified in our survey:
Optogenetics
Optogenetics represents a significant leap forward in ophthalmic therapeutics, offering a potential solution for vision restoration in patients with advanced retinal degenerative diseases, where traditional gene therapy often falls short. While gene replacement therapies are constrained by the need for viable target cells and the complexity of multi-gene disorders like retinitis pigmentosa (RP), optogenetics offers a broader approach.
This technique aims to circumvent the loss of photoreceptors by introducing light-sensitive proteins, known as opsins, into the surviving inner retinal cells and optic nerve, restoring visual function through light modulation. This method is particularly advantageous as it is agnostic to the specific genetic cause of retinal degeneration.
By delivering opsin genes to retinal neurons, the technology enables the precise manipulation of cellular activity, essentially transforming these cells into new light-sensing units. This approach can bypass the damaged photoreceptor layer, transmitting visual signals directly to the brain.
Several companies are pioneering advancements in this field. RhyGaze, for example, has secured substantial funding to accelerate the development of its lead clinical candidate, a novel gene therapy designed for optogenetic vision restoration. Their efforts encompass preclinical testing, including pharmacology and toxicology studies, an observational study to define clinical endpoints, and a first-in-human trial to assess safety and efficacy. The success of RhyGaze’s research could pave the way for widespread clinical applications, significantly impacting the treatment of blindness globally.
Nanoscope Therapeutics is also making significant strides with its MCO-010 therapy. This investigational treatment, administered through a single intravitreal injection, delivers the Multi-Characteristic Opsin (MCO) gene, enabling remaining retinal cells to function as new light-sensing cells. Unlike earlier optogenetic therapies that required bulky external devices, MCO-010 eliminates the need for high-tech goggles, simplifying the treatment process and enhancing patient convenience. The ability to restore light sensitivity without external devices represents a major advancement, potentially broadening the applicability of optogenetics to a wider patient population.
Another critical area of innovation highlighted in our survey is the advancement of treatments for AMD and GA.
New AMD/GA Treatment
Age-related macular degeneration (AMD) and geographic atrophy (GA) represent a significant challenge in ophthalmology, demanding innovative therapeutic strategies beyond the established anti-VEGF paradigm.
Gene Correction
Gene editing is emerging as a powerful tool in the fight against AMD and GA, potentially correcting the underlying genetic errors that contribute to these diseases. Essentially, it allows us to make precise changes to a patient’s DNA.
Traditional gene editing techniques often rely on creating ‘double-strand breaks’ (DSBs) in the DNA at specific target sites, which are like precise cuts in the DNA strand. These cuts are made using specialized enzymes, like CRISPR-Cas9, which act as molecular scissors. While effective, these methods can sometimes introduce unwanted changes at the cut site, such as small insertions or deletions.
After a DSB is made, the cell’s natural repair mechanisms kick in. There are two main pathways:
- Non-Homologous End Joining (NHEJ): This is the cell’s quick-fix method. It essentially glues the broken ends back together. However, this process can sometimes introduce errors, leading to small insertions or deletions that can disrupt the gene’s function.
- Homology-Directed Repair (HDR): This is a more precise repair method. It uses a ‘donor’ DNA template to guide the repair process, ensuring accuracy. However, HDR is more complex and less efficient, especially in non-dividing cells.
To overcome these limitations of traditional gene editing, researchers have developed more precise techniques:
- Base Editing: This technique allows scientists to change a single ‘letter’ in the DNA code without creating DSBs.
- Prime Editing: This advanced technique builds upon CRISPR-Cas9, allowing for a wider range of precise DNA changes. It can correct most disease-causing mutations with enhanced safety and accuracy.
- CASTs (CRISPR-associated transposases): This method enables larger DNA modifications without creating DSBs, offering a safer approach to genetic correction.
Why does this matter for AMD and GA? These advancements in gene editing are crucial for addressing the genetic roots of these pathologies. We can potentially develop more effective and targeted therapies by precisely correcting the faulty genes that contribute to these diseases. The technologies are still being researched, but they hold great promise for the future of ophthalmology.
Cell Reprogramming
Cell reprogramming offers a novel approach to regenerative medicine, with the potential to replace damaged retinal cells. This technique involves changing a cell’s fate, either in vitro or in vivo. In vitro reprogramming involves extracting cells, reprogramming them in a laboratory, and then transplanting them back into the patient. In vivo reprogramming, which directly reprograms cells within the body, holds particular promise for retinal diseases. This approach has succeeded in preclinical studies, demonstrating the potential to restore vision in conditions like congenital blindness.
Vectors and Delivery Methods
The success of gene therapy relies on efficiently delivering therapeutic genes to target retinal cells. Vectors are essentially delivery vehicles, designed to carry therapeutic genes into cells. These vectors can be broadly classified into two categories: viral and non-viral. Vectors, both viral and non-viral, are crucial for this process.
Viral vectors are modified viruses that have been engineered to remove their harmful components and replace them with therapeutic genes. They are highly efficient at delivering genes into cells, as they have evolved to do just that. Adeno-associated viruses (AAVs) are the most commonly used viral vectors in ocular gene therapy due to their safety profile and cell-specificity. The diversity of AAV serotypes allows for tailored gene delivery to specific retinal cell types.
Non-viral vectors, on the other hand, are synthetic systems that don’t rely on viruses. They can be made from lipids, polymers, or even DNA itself. While they may be less efficient than viral vectors, they offer safety and ease of production advantages.
Advances in vector design, whether viral or non-viral, are focused on enhancing gene expression, cell-specificity, and carrying capacity.
Now, let’s examine the ongoing evolution of anti-VEGF treatments, a cornerstone of modern retinal care.
New Anti-VEGF drugs
The landscape of ophthalmology has undergone a dramatic transformation since the early 1970s when Judah Folkman first proposed the concept of tumor angiogenesis. His idea sparked research that ultimately led to the identification of vascular endothelial growth factor (VEGF) in 1989 and the development of anti-VEGF therapies, revolutionizing the treatment of neovascular eye diseases, dramatically improving outcomes for patients with wet AMD, diabetic retinopathy, and retinal vein occlusions.
Population-based studies have shown a substantial reduction (up to 47%) in blindness due to wet AMD since the introduction of anti-VEGF therapies. However, significant gaps remain despite this progress, especially regarding treatment durability. Anti-VEGF drugs require frequent intravitreal injections, which can be difficult for patients due to time commitments, financial costs, and potential discomfort. Although newer agents have extended treatment intervals, patient adherence and undertreatment challenges persist in real-world settings. Innovative approaches are being investigated to address these unmet needs to increase drug durability and reduce the treatment burden.
Tyrosine Kinase Inhibitors
One approach to increasing treatment durability is using tyrosine kinase inhibitors (TKIs). TKIs are small-molecule drugs that act as pan-VEGF blockers by binding directly to VEGF receptor sites inside cells, offering a different action mechanism than traditional anti-VEGF drugs that target circulating VEGF proteins.
Currently, TKIs are being investigated as maintenance therapy, primarily in conjunction with sustained-release delivery systems. Two promising TKIs for retinal diseases are axitinib and vorolanib. In a bioresorbable hydrogel implant, Axitinib is being studied for neovascular AMD and diabetic retinopathy. Vorolanib, in a sustained-release delivery system, is also being investigated for neovascular AMD. These TKIs offer the potential for less frequent dosing, reducing the treatment burden for patients.
Port Delivery System
The Port Delivery System (PDS) is a surgically implanted, refillable device that provides continuous ranibizumab delivery for up to 6 months. While it’s FDA-approved for neovascular AMD, it’s also being investigated for other retinal diseases, such as diabetic macular edema and diabetic retinopathy.
Although the PDS faced a voluntary recall due to issues with septum dislodgment, it has returned to the market with modifications. The PDS offers the potential for significantly reduced treatment frequency for a subset of patients. However, challenges remain, including the need for meticulous surgical implantation and the risk of endophthalmitis.
Nanotechnology
Nanotechnology offers promising solutions to overcome limitations of current ocular drug delivery. The unique structure of the eye, with its various barriers, poses challenges for drug delivery. Topical administration often fails to achieve therapeutic concentrations, while frequent intravitreal injections carry risks. Nanotechnology can improve drug solubility, permeation, and bioavailability through nanoparticles, potentially extending drug residence time and reducing the need for frequent injections. Several nanoparticle systems, lipid and polymeric, are being studied for ocular drug delivery, offering hope for more effective and less invasive treatments.
FDA-cleared AI for OCT analysis
Summing up
The advancements discussed in this article, encompassing AI, optogenetics, novel AMD/GA therapies, and refined anti-VEGF treatments, collectively signal a transformative era for ophthalmology. As highlighted by the survey results, AI probably encompasses most of the changes by redefining diagnostic and clinical workflows through its capacity for image analysis, biomarker identification, and personalized patient management.
Optogenetics offers a distinct pathway to vision restoration, bypassing limitations of traditional gene therapy. The progress in AMD/GA treatments, particularly gene editing and cell reprogramming, presents opportunities for targeted interventions. Finally, the evolution of anti-VEGF therapies, with innovations in drug delivery and sustained-release mechanisms, addresses persistent challenges in managing neovascular diseases.
These developments, driven by technological innovation and clinical research, promise to enhance patient outcomes and reshape the future of ophthalmic care.
-
Altris AI Launches Advanced Optic Disc Analysis for Glaucoma, Complementing GCC Asymmetry Analysis
Maria Znamenska
1 min.Altris AI, a leading force in AI for OCT scan analysis that detects the widest range of retina pathologies and biomarkers, launches an advanced glaucoma Optic Disc Analysis module.
Early detection of glaucoma demands exceptional precision, as the early signs are often subtle and difficult to detect. A major challenge in glaucoma screening is the high rate of false positive referrals, which can lead to unnecessary appointments in secondary care. This not only burdens healthcare systems but also causes anxiety for patients. Yet delayed or missed detection of glaucoma results in irreversible vision loss for millions of people worldwide. So the need for timely and accurate glaucoma detection has never been so critical in the eye care industry, and automated AI-powered glaucoma analysis will offer a transformative potential to improve outcomes.
To address this critical need, Altris AI has introduced its Advanced Optic Disc (OD) Analysis, building on its earlier innovation with Ganglion Cell Complex (GCC) Asymmetry Analysis to enhance the improvements from the Altris AI macula module which has been available for several years.
Altris AI’s glaucoma detection journey began with the creation of AI-powered GCC Asymmetry Analysis, designed to detect early risk of glaucoma.
In February 2025 Altris launched the AI-powered Advanced Optic Disc (OD) Analysis module as OD analysis is regarded as the gold standard for structural glaucoma diagnosis.
This method provides a comprehensive picture of structural damage and allows detailed glaucoma assessment for treatment choice and monitoring.
The module evaluates optic disc parameters using OCT, providing personalized assessments by accounting for individual disc sizes and angle of rim absence. This tailored approach eliminates reliance on normative databases, making evaluations more accurate and patient-specific.
Altris AI’s platform assigns a severity score for optic disc damage on a scale from 1 to 10, offering valuable insights into glaucomatous changes. Furthermore, it enables cross-evaluation across different OCT systems, allowing practitioners to analyze both macula and optic disc pathology, even when data originates from multiple OCT devices.
Optic Disc Analysis for Glaucoma: Key Parameters
- Disc area
- Cup area
- Cup volume
- Minimal Cup depth
- Maximum Cup depth
- Cup/Disc area ratio
- Rim Absence angle
- Disc-Damage Likelihood Scale (DDLS)
The Altris AI Glaucoma Module is compatible with various OCT scan protocols, including:
- 3D OCT optic disc scans
- 3D OCT horizontal wide scans
- 3D OCT vertical-wide scans
- OCT optic disc raster scans
By combining GCC Asymmetry and Advanced Optic Disc analysis for glaucoma empower enabling Eyecare practitioners (ECPs) to make faster evaluations and explore a wider range of treatment options. This streamlined approach empowers ECPswith timely, actionable data, ultimately improving patient outcomes and care.
Dr. Maria Znamenska, MD, PhD, and a Chief Medical Officer at Altris AI, commented:
“The launch of our Advanced Optic Disc Analysis module marks a pivotal step forward in glaucoma care. By combining the gold standard of optic disc evaluation with AI-powered precision, we’re equipping eye care professionals with the tools to make more accurate and timely diagnosis of this vision-threatening disorder. This innovation not only reduces false positive referrals but also enhances early detection and treatment planning—ensuring better outcomes for patients and optimizing healthcare resources. Together with GCC asymmetry analysis, our platform empowers clinicians to elevate the standard of glaucoma care, offering hope to millions at risk of vision loss.”
About Altris AI
Altris AI is an artificial intelligence platform for OCT analysis, capable of detecting the widest range of retinal pathologies and biomarkers on the market – more than 70. Leading the way in AI innovation, Altris AI provides transformative solutions that enhance the diagnosis, treatment, and monitoring of retinal diseases, enabling eye care professionals to deliver exceptional patient care.
-
ML Applied to 3D Optic Disc Analysis for Glaucoma Risk Assessment Across Different OCT Scan Protocols Without a Normative Database
Angelina Hramatik
14.02.202520 min readMachine Learning Applied to 3D Optic Disc Analysis for Glaucoma Risk Assessment Across Different OCT Scan Protocols Without a Normative Database
1. Introduction
Glaucoma is one of the leading causes of irreversible blindness worldwide, affecting millions of people annually. The disease is often asymptomatic in its early stages, making timely diagnosis particularly challenging. Early detection of glaucomatous changes is crucial for preventing vision loss and improving long-term patient outcomes.
One well-established method for assessing glaucoma is the Disc Damage Likelihood Scale (DDLS), which evaluates structural changes in the optic nerve head (ONH) based on the extent of neuroretinal rim loss. This method categorizes glaucomatous damage severity by analyzing the relationship between the optic cup and neural rim, while also accounting for optic disc size without relying on a normative database. 1, 2, 3, 4.
While DDLS is recognized for its reliability and utility in clinical practice, it is not a standalone diagnostic tool. Rather, it is one of several methods used to identify signs of glaucoma, and its implementation is often limited to specific imaging modalities or scan protocols, such as 3D optic disc-only scans or fundus images.
In this article, we introduce an enhanced approach to DDLS analysis that overcomes these limitations. We want to present a solution, which is capable of performing DDLS analysis on any OCT scan protocol that captures the optic nerve, including 3D optic disc scans (which provide the most detailed view of the nerve), as well as OCT horizontal and vertical 3D wide scans. By leveraging advanced machine learning models, we achieve unprecedented flexibility and accuracy, ensuring reliable analysis across different scanning protocols and OCT systems.
Unlike traditional systems restricted to specific devices or data formats, our solution processes scans from multiple OCT systems. Moreover, it excels in challenging scenarios, providing clinicians with a robust and versatile tool for analyzing potential signs of glaucoma.
FDA-cleared AI for OCT analysis
A Brief Theoretical Overview
Optical coherence tomography (OCT) scans vary in the anatomical regions they capture. One specific type is the optic disc OCT scan (Figure 2), which provides high-resolution imaging of the optic disc and the surrounding optic nerve head (ONH) structures. This scan type is commonly used in glaucoma assessment, as it allows for the evaluation of the optic nerve’s structure, including the neuroretinal rim, optic cup, and surrounding peripapillary retinal nerve fiber layer (RNFL) — key areas affected in glaucomatous damage.
Figure 1. Photograph of the retina of the human eye, with overlay diagrams showing the positions and sizes of the macula, fovea, and optic disc (Reference).
Figure 2. 6 mm OCT b-scan of the optic nerve head (ONH) region.
In contrast, macular OCT scans (Figure 3) focus on the central retina, providing detailed visualization of structures such as the foveal center, retinal layers, and macular biomarkers (such as drusen, hypertransmission, fluids etc). Since the macula is anatomically distinct from the optic nerve head, standard macular scans do not capture the ONH comprehensively.
Figure 3. 6 mm OCT b-scan of the macular region, showing the foveal pit and retinal layers.
A more comprehensive scanning approach is 12 mm wide scan OCT (Figure 4), which captures both the macular region and optic nerve head in a single scan. This broader field of view allows for the simultaneous assessment of central retinal structures and optic nerve-related changes, making it valuable for detecting and monitoring conditions that affect both regions, such as glaucoma and other neurodegenerative or vascular retinal diseases.
Figure 4. 12 mm wide scan OCT b-scan, which captures both the macular region and part of the optic nerve head.
2. Results
2.1. Experiment Setup
Brief Method Overview
To evaluate the effectiveness of DDLS analysis in assessing glaucoma severity, we designed an experiment comparing results obtained from processing 3D Optic Disc OCT scans and 3D Wide scan OCT scans with the corresponding reports generated by the OCT system. Our method follows four key steps:
- Detecting optic nerve landmarks like Bruch’s Membrane Opening (BMO) points (Eye Keypoints Retrieval / OCT Keypoint Detector Model);
- Segmenting the inner limiting membrane (ILM) (Retina Layers Segmentation Model);
- Reconstructing the neuroretinal rim geometry;
- Applying the Disc Damage Likelihood Scale (DDLS) for classification.
The dataset below was used to validate the algorithm.
Dataset Used for Validating the Entire Algorithm
For validation, we compared our algorithm’s DDLS measurements with the DDLS values generated by the built-in algorithms of the Optopol REVO NX 130 OCT system. This provided a baseline for assessing accuracy and consistency.
To validate our approach, we conducted an experiment comparing DDLS metrics derived from:
- 3D Optic Disc OCT scans, which are traditionally used for DDLS analysis.
- 3D Wide scans, which capture both the macular and optic nerve regions, providing a more comprehensive dataset for analysis.
The dataset includes imaging data from 37 patients examined using the Optopol REVO NX 130 OCT system, with each patient undergoing the following protocols on the same day:
- 3D Optic Disc OCT (6mm zone): 168 scans
- 3D Wide scan (horizontal protocol, 12mm): 128 scans
A report was obtained from the 3D Optic Disc OCT scans, containing all parameters calculated by the device.
Since no manual annotations are available for these data, our comparison is conducted directly against the device-generated results.
The distribution of data was as follows:
- Glaucomatous Optic Disc: 21 cases;
- Normal Optic Disc: 16 cases.
2.2. Final Validation Results: DDLS Accuracy and Error Metrics
To evaluate the performance of our DDLS analysis method, we compared its results with the corresponding DDLS values generated by the OCT device’s built-in algorithms. The device reports serve as a reference point for all calculations, meaning the accuracy, MAE/STD values presented below indicate the level of agreement between our method and the device’s measurements.
The parameters compared below are the key indicators for glaucoma stage assessment.
- The rim-to-disc ratio (RDR) represents the thinnest neuroretinal rim width relative to the vertical optic disc diameter. A lower RDR indicates a more advanced stage of rim thinning, as glaucoma leads to progressive narrowing of the neuroretinal rim due to the loss of ganglion cells axons.
- The rim absence angle (RAA) quantifies the extent of neuroretinal rim loss in degrees. It defines the angle where the rim is completely absent, exposing the optic cup. A wider RAA suggests a more severe stage of glaucoma, as it indicates greater rim loss across the disc circumference.
Both RDR and RAA provide complementary perspectives on structural optic nerve damage:
- RDR measures the smallest remaining rim thickness in proportion to the disc.
- RAA evaluates how much of the disc circumference has lost its rim.
By considering both parameters together, a more comprehensive assessment of glaucoma severity can be achieved. Based on RDR and RAA, a DDLS stage is assigned, allowing for standardized classification of glaucoma progression.
Table 1. Validation Results of DDLS Analysis on 3D Optic Disc and 3D Wide Scan OCT Scans
The table presents validation results comparing 3D Optic Disc OCT scan and 3D Wide scan OCT in DDLS analysis, focusing on Mean Absolute Error (MAE) and Standard Deviation (STD) for key parameters, along with overall DDLS staging accuracy. These metrics are calculated for the rim-to-disc ratio and rim absence angle by comparing their respective values from 3D Optic Disc OCT scans and 3D Wide scans against those from the device reports, providing a precise assessment of deviations from the reference values.
Key Observations
1. Our Goal: Consistency with Device Reports, Not Outperformance
The experiment does not aim to surpass the device’s accuracy but rather to demonstrate that our method produces results in alignment with the device-generated DDLS reports.
The device report serves as a reference, helping to interpret the figures we present, but this does not mean the device’s output is always the absolute truth.
2. High DDLS Staging Accuracy for Both Scan Types
3D Optic Disc OCT scan: 97.3% accuracy in determining DDLS glaucoma stage.
3D Wide scan OCT: 94.59% accuracy, demonstrating strong reliability despite a broader scan area and fewer scans capturing the nerve, leading to less available information.
Conclusion:
- Both types of scans allow the production of clinically reliable DDLS results, but as expected, 3D optic disc scans provide slightly better accuracy due to their higher resolution of the optic nerve head (ONH).
- The small accuracy gap and close values for key parameters between the two suggests that 3D wide scan OCT can still be a viable option for glaucoma assessment, despite offering less detailed information about the optic nerve compared to optic disc scans.
3. RD Ratio and Rim Absence Angle: High Precision Within Clinical Margins
RD Ratio (rim-to-disc ratio):
- Step size between DDLS stages: 0.1.
- Mean Absolute Error (3D Optic Disc OCT scan): 0.008 (significantly smaller than step size).
- Mean Absolute Error (3D Wide scan OCT): 0.024 (still relatively small).
Conclusion:
- Both 3D Optic Disc OCT scan and 3D Wide scan analysis provide high precision in RD ratio calculations.
- The small error ensures that stage classification remains reliable, especially in optic disc scans.
Rim Absence Angle:
- Step size between DDLS stages: Minimum 45°.
- Mean Absolute Error (3D Optic Disc OCT scan): 2.2° (very small compared to step size). Mean Absolute Error (3D Wide scan OCT): 4.2° (still well below stage transition threshold).
Conclusion:
- The method’s margin of error is far smaller than the clinical threshold for stage differentiation, confirming high accuracy in rim loss assessment.
- 3D Optic Disc scans again show better precision, reinforcing that they remain the preferred scan type for DDLS.
4. Our Advantage: Ability to Perform DDLS on Both Scan Types
- Unlike traditional DDLS implementations, which work only with 3D Optic Disc scans, our method can perform DDLS analysis on both 3D Wide scan and 3D Optic Disc OCTs.
- However, 3D Optic Disc OCT remains the preferred method for maximum precision, as it provides a higher-resolution view of the optic nerve.
Key Conclusions
- Our method is unique in its ability to process multiple scan types, while still maintaining high accuracy in both cases.
- On 3D Optic Disc scans, we achieve maximum precision, while on 3D Wide scans, we still maintain clinically reliable accuracy.
- Consistency: Across all glaucoma stages, our method produced stable results that closely matched ground truths provided by medical experts.
- Universal Compatibility: The algorithm performed equally well with scans from other manufacturers, demonstrating its versatility and robustness.
2.3. Patient Case Studies: DDLS Analysis in Real-World Scenarios
Accurate assessment of glaucoma severity relies on precise measurements of optic nerve parameters, such as disc area, rim-to-disc ratio, and rim absence angle. In the following examples, we analyzed four patient cases, including both normal optic discs and glaucomatous eyes, using 3D Optic Disc OCT scan, 3D Wide scan OCT, and device-generated reports as a reference standard.
By consolidating individual patient cases into a single comparative table, we can examine the consistency of DDLS analysis across different scan types and highlight key variations that may arise due to differences in scan coverage, segmentation accuracy, and anatomical structure. The following table summarizes the key optic nerve parameters measured for each patient and scan type.
Table 2. Comparative DDLS Evaluation Across Multiple Patient Cases
Key Findings & Interpretation
1. High Consistency Between Our Method and Device Reports
- Across all cases, the DDLS stage remains identical (4 for normal eyes, 7 or 8 for glaucomatous cases) regardless of whether the input scan was 3D Optic Disc OCT or wide scan, and this result corresponds to the device-generated report.
- Key optic nerve parameters such as disc area, cup area, and rim area closely align with the device reference, demonstrating strong algorithm performance.
2. Minor Variations in Cup and Rim Measurements
- Cup and rim area values show slight deviations between 3D Optic Disc OCT scans and 3D Wide scan scans, which is expected due to differences in scan coverage and segmentation sensitivity.
- For example, in Patient 3 (Glaucoma, Stage 8):
- Cup area was 1.86 mm² (3D Optic Disc OCT scan), 1.88 mm² (3D Wide scan), and 1.81 mm² (Device Report).
- Rim area was 0.55 mm² (3D Optic Disc OCT scan), 0.53 mm² (3D Wide scan), and 0.58 mm² (Device Report).
- These small variations do not affect final DDLS staging but highlight how scan type can introduce subtle segmentation differences.
3. Rim Absence Angle Varies Slightly but Remains Within Expected Tolerances
- The rim absence angle shows minor fluctuations across scan types, especially in glaucomatous cases.
- Example: In Patient 3 (Stage 8 Glaucoma), the device reported a rim absence angle of 162°, while our algorithm calculated 155° (3D Optic Disc OCT scan) and 151° (3D Wide scan).
- Since DDLS categories for severe glaucoma are defined in large increments (e.g., 45°+ thresholds), these small differences do not impact staging accuracy.
4. 3D Wide scan OCT Provides Comparable Results to 3D Optic Disc OCT scan
- Despite covering a larger field of view, wide scans produced DDLS staging results consistent with 3D Optic Disc OCT scans and device reports.
- In patients with coexisting macular pathologies, 3D Wide scan OCT may provide additional clinical insights while still maintaining high reliability for glaucoma staging.
Conclusion: Reliable DDLS Analysis Across Different Scan Types
This unified case study analysis confirms that our DDLS analysis algorithm produces highly consistent results across different scan protocols and patient conditions.
- DDLS stage assignment is identical to device reports across all scan types, ensuring high agreement with clinically validated reference values.
- Key optic nerve measurements (disc area, cup area, rim area) are closely aligned across 3D Optic Disc OCT scan, 3D Wide scan, and device reports, reinforcing algorithm accuracy.
- Minor variations in rim absence angle and segmentation metrics do not affect final glaucoma staging, highlighting the algorithm’s robustness.
- 3D Wide scan OCT offers a viable alternative for 3D Optic Disc OCT scans, particularly in cases where both macular and optic nerve regions need simultaneous evaluation.
5. Visual Comparison Shows Strong Similarity to Device Reports
- The disk and cup boundaries detected by our algorithm closely match those in the device-generated reports, maintaining consistent shapes and anatomical alignment across both 3D Optic Disc and 3D Wide scan OCT scans.
- However, wide scan-based segmentations tend to be slightly rougher, as less structural information is available compared to dedicated optic disc scans. This trade-off is expected due to the broader field of view in wide scans.
These findings validate our algorithm’s flexibility, adaptability, and clinical reliability, demonstrating its potential for seamless integration into real-world ophthalmic workflows.
2.4. Why Our Approach Stands Out: Key Advantages Over Traditional DDLS Systems
While the previous patient case studies demonstrated the accuracy and consistency of our DDLS analysis across different optic disc conditions, another critical advantage of our method is its ability to work seamlessly across various scanning protocols. Unlike traditional device-restricted solutions, our approach supports DDLS assessment on both standard 3D Optic Disc OCT scans and 3D Wide scans with different orientations.
The following table illustrates the same patient’s optic nerve head analyzed using three different scanning protocols: 3D Optic Disc OCT scan, 3D Wide scan Horizontal, and 3D Wide scan Vertical. This comparison highlights the method’s adaptability to different scan formats, ensuring reliable DDLS analysis regardless of the scanning protocol used. This example is taken from a Topcon Maestro 2 OCT system, providing an additional reference for processing across different OCT systems.
Table 3. Comparative DDLS Analysis Across Different Scanning Protocols: 3D Optic Disc OCT, 3D Wide scan Horizontal, and 3D Wide scan Vertical.
This capability significantly enhances clinical applicability, allowing our algorithm to process data from various scanning protocols and devices while maintaining high accuracy. The ability to analyze both 3D Optic Disc and 3D Wide scan OCT scans — across different orientations and machine types — ensures comprehensive glaucoma assessment even in cases where scan availability or quality may vary.
Key advantages over traditional DDLS analysis methods
1. Device Independence
- While most existing solutions are restricted to proprietary OCT data formats, our algorithm processes scans from any OCT system, ensuring broad compatibility across devices.
2. Consistent Accuracy Across Different Scan Types
- Our algorithm closely matches device-generated DDLS reports, achieving 97.3% accuracy for 3D Optic Disc OCT scans and 94.59% for 3D Wide scan OCTs.
- Patient cases confirm this consistency, with both normal and glaucomatous eyes correctly classified, even when analyzed with different scan types.
3. Robust Performance in Edge Cases
- Unlike traditional device-based DDLS assessments, which may struggle with low-quality images or atypical anatomical features, our approach maintains high accuracy in challenging clinical scenarios.
- Patient examples with small optic discs and advanced-stage glaucoma demonstrated that our algorithm successfully identified key DDLS indicators even when scan quality or nerve structure was less distinct.
4. Expanded Assessment Through 3D Wide scan OCT
- The ability to perform DDLS analysis on Horizontal and Vertical 3D Wide scans allows for a more comprehensive evaluation by incorporating both macular and optic nerve data.
- In patients with coexisting macular pathologies, wide scans enabled earlier detection of glaucomatous changes that would have been missed if only optic disc scans were used.
3. Detailed Approach Description
To assess glaucoma stage on OCT scans using DDLS analysis, the following steps should be performed:
- Optic Nerve Landmarks Detection – Localization of the optic nerve in the b-scan view of each scan by identifying key anatomical landmarks.
- ILM Detection – Segmentation of the inner limiting membrane (ILM) in the b-scan view of each scan to establish a reference for neuroretinal rim measurement.
- Neuroretinal Rim Reconstruction – Construction of the neuroretinal rim geometry based on detected nerve landmarks and ILM segmentation.
- DDLS Analysis – Application of the Disc Damage Likelihood Scale (DDLS) to assess glaucoma severity based on neuroretinal rim measurements. This includes assigning a DDLS stage according to rim width and optic disc size, with a focus on detecting localized thinning and asymmetry.
3.1. Keypoint Annotation Process / Nerve Detection
The foundation of our approach lies in a high-quality, annotated dataset meticulously labeled by a team of four expert ophthalmologists. The annotation process focused on identifying key anatomical landmarks in both the macular region and the optic disc nerve zones, both of which are critical for detecting glaucomatous changes and performing Disc Damage Likelihood Scale (DDLS) analysis.
These keypoints serve as essential data for evaluating disease progression and training machine learning models. The dataset was carefully selected based on key clinical features, such as the presence or absence of nerve fibers, foveal pits, and other pathological markers, ensuring a comprehensive representation of various conditions and scan types.
The annotated dataset consists of approximately 370 unique OCT examinations with more than 56,000 b-scans, covering a range of physical scanning areas, pathology types, and optic nerve conditions to enhance the model’s robustness. The scans are categorized as follows:
- Optic Disc with no excavation: ~15 examinations;
- Glaucomatous Optic Disc: ~105 examinations;
- Normal Optic Disc: ~105 examinations;
- Wide scans (covering both the macular and optic nerve regions): ~60 examinations;
- Normal Retina Scans: ~40 examinations;
- Pathological Retina Scans: ~45 examinations.
This detailed annotation process ensures high precision and reliability, enabling the algorithm to generalize across diverse cases while maintaining clinical accuracy in real-world scenarios.
3.2. Eye Keypoints Retrieval / OCT Keypoint Detector
Our keypoint detection model represents a logical evolution of the model for exam center detection, designed to efficiently and accurately identify key anatomical landmarks in OCT scans. The architecture integrates elements from UNet 5 and CenterNet 6, incorporating YOLO-inspired 7 techniques for keypoint prediction. Additionally, the backbone has been adapted to a transformer-based model 8, enhancing feature extraction capabilities.
Training Process
The training process follows a multi-stage approach, ensuring robustness, accuracy, and efficiency:
- Stage 1: Detects general keypoints, establishing a foundation for precise landmark localization.
- Stage 2: Groups and refines the identification of specific keypoints, progressively improving the model’s understanding of anatomical structures.
This structured approach enhances the model’s reliability across different scan types while maintaining computational efficiency.
Key Features
Data Preprocessing
- The data is augmented using unsupervised techniques, leveraging libraries such as Albumentations 9 to introduce variations such as rotations, scaling, and noise addition.
- This ensures the model encounters a wider variety of real-world scenarios during training, improving its generalization capability.
Training Process
- The model is trained using supervised learning techniques, optimizing a loss function through backpropagation and gradient descent.
- This approach allows for continuous refinement and adaptation to complex variations in OCT scans.
Parameterization & Tuning
- The model includes millions of adjustable parameters (weights), which are fine-tuned to increase accuracy.
- Key hyperparameters such as learning rate, batch size, and network depth are carefully selected to maximize performance.
- Advanced optimization techniques, including grid search, random search, and Bayesian optimization, are used to find the best hyperparameter configuration.
3.3. Retina Layers Segmentation Model
The Retina Layers Segmentation Model is our production-stage model, actively used within the Altris AI platform. It was incorporated into this experiment without modifications, ensuring that the results reflect real-world performance as seen in our deployed system.
Our Retina Layers Segmentation Model enables precise segmentation of key retinal layers in OCT scans, crucial for detecting structural changes linked to glaucoma and other retinal diseases. The model identifies:
- ILM, RNFL, GCL, IPL, INL, OPL, ONL, ELM, MZ, EZ, OS, RPE, BM
The training dataset consists of 5,000 expert-annotated OCT b-scans, covering a diverse range of patient demographics, including different ages and ethnic backgrounds. The segmentation model is designed to detect and delineate key retinal layers with high accuracy.
Training & Architecture
The model is based on U-Net with a ResNet backbone, optimized for OCT images. Training includes:
- Expert Annotation: Medical specialists labeled layers for ground truth.
- Augmentation: Albumentations-based transformations enhance robustness.
- Supervised Learning: Predicts segmentation masks using backpropagation.
- Hyperparameter Optimization: Grid search, random search, and Bayesian tuning maximize performance.
Model Validation & Performance
- The model was validated using a holdout validation approach, with separate validation and test sets that were not exposed during training.
- Real-world testing was conducted using scans from various clinical settings to ensure robustness.
- Performance was evaluated using the Mean Dice Coefficient across all layers, achieving a score of 0.80, with layer-specific scores ranging from 0.63 to 0.92, confirming high segmentation accuracy.
- Cross-domain testing demonstrated consistent performance across different OCT systems, and stability was confirmed over scans collected across different time periods.
This efficient, accurate, and generalizable model strengthens DDLS analysis and enhances AI-driven retinal diagnostics.
3.4. DDLS Algorithm
The DDLS algorithm evaluates glaucomatous changes by analyzing the geometric relationship between the neural rim and optic cup in the optic nerve head. Key steps include:
- Localization: Identifying boundaries of the optic cup and neuroretinal rim by reconstructing geometry on a b-scan view using disc landmarks and an inner limiting membrane.
Figure 5. B-scan Geometry Visualization.
- Measurement: Calculating the DDLS stage based on the ratio between the rim and disc boundaries.
- Cross-Scan Application: Adapting the analysis for 3D Wide scans (both Horizontal and Vertical protocols) as well as 3D Optic Disc-specific scans.
Our implementation enhances this traditional method by leveraging wide scans, enabling a more comprehensive assessment of glaucomatous changes.
3.5. Evaluation
To ensure the reliability and effectiveness of our DDLS algorithm, we conducted a rigorous evaluation process, adhering to best practices in data usage, ethics, and performance validation.
Data Integrity
- Measures were implemented to prevent data leakage, ensuring that scans from the same patient did not appear in both training and testing sets.
Ethical Considerations
- The analysis strictly relies on OCT-related data (e.g., scan zone size, laterality, pixel spacing) without incorporating any personal patient information.
Performance Metrics
- Keypoint detection accuracy was evaluated using Mean Squared Error (MSE), comparing model-predicted keypoints with expert annotations.
- Additional metrics included correctness of scan center-related landmarks and accuracy in the optic nerve region, ensuring precision in clinical applications.
The evaluation results confirmed the algorithm’s robustness, demonstrating significant performance gains, particularly in edge cases, where traditional methods often struggle.
Discussion
Our DDLS analysis method represents a significant advancement in glaucoma detection. Key benefits include:
- Universal Compatibility: The ability to process data from various devices ensures broad applicability.
- Enhanced Accuracy: By incorporating data from both macular and optic nerve regions, our approach captures more subtle glaucomatous changes.
- Edge Case Performance: Advanced machine learning techniques enable accurate analysis even in challenging scenarios.
Compared to traditional methods, our system provides a more flexible, reliable, and comprehensive solution for early glaucoma detection.
FDA-cleared AI for OCT analysis
Conclusion
By integrating 3D Wide scans and state-of-the-art machine learning models, we have enhanced DDLS analysis for glaucoma detection, ensuring high accuracy, broad compatibility, and robustness across diverse clinical scenarios.
Unlike traditional solutions, our algorithm:
- Works across multiple OCT devices, eliminating the constraints of proprietary data formats.
- It closely matches device-generated DDLS reports, achieving 97.3% accuracy for 3D Optic Disc OCT scans and 94.59% for 3D Wide scans.
- Performs reliably in edge cases, such as small optic discs and advanced-stage glaucoma, where traditional methods may struggle.
- Supports both Horizontal and Vertical 3D Wide scans, enabling more comprehensive assessments that incorporate both macular and optic nerve data.
- Enhances early glaucoma detection, particularly in patients with coexisting macular pathologies, where wide scans provide additional clinical insights.
By delivering consistently accurate DDLS staging, regardless of scan type or manufacturer, our system establishes a new benchmark for universal glaucoma assessment. This technology has the potential to significantly improve early detection and management, ultimately preserving vision and enhancing patient outcomes.
References
- Spaeth, G. L. (2005). The Disc Damage Likelihood Scale. Glaucoma Today. https://glaucomatoday.com/articles/2005-jan-feb/0105_18.html
- Cheng, K. K. W., & Tatham, A. J. (2021). Spotlight on the Disc-Damage Likelihood Scale (DDLS). Clinical Ophthalmology, 15, 4059–4071. https://pmc.ncbi.nlm.nih.gov/articles/PMC8504474/
- Zangalli, C., Gupta, S. R., & Spaeth, G. L. (2011). The disc as the basis of treatment for glaucoma. Saudi Journal of Ophthalmology, 25(4), 381-387. https://www.sciencedirect.com/science/article/pii/S1319453411000993
- Review of Optometry Staff. (2023, January 23). Optic disc staging systems effective in grading advanced glaucoma. Review of Optometry. https://www.reviewofoptometry.com/article/optic-disc-staging-systems-effective-in-grading-advanced-glaucoma
- Ronneberger O, Fischer P, Brox T. U-Net: Convolutional Networks for Biomedical Image Segmentation. [Preprint]. Posted May 18, 2015. https://arxiv.org/abs/1505.04597
- Duan K, Bai S, Xie L, et al. CenterNet: Keypoint Triplets for Object Detection. [Preprint]. Posted April 17, 2019. https://arxiv.org/abs/1904.08189
- Redmon J, Divvala S, Girshick R, Farhadi A. You Only Look Once: Unified, Real-Time Object Detection. [Preprint]. Posted June 8, 2015. https://arxiv.org/abs/1506.02640
- Dosovitskiy A, Beyer L, Kolesnikov A, et al. An Image is Worth 16×16 Words: Transformers for Image Recognition at Scale. [Preprint]. Posted October 22, 2020. https://arxiv.org/abs/2010.11929
- Buslaev A, Iglovikov V, Khvedchenya E, et al. Albumentations: Fast and Flexible Image Augmentations. [Preprint]. Posted September 18, 2018. https://arxiv.org/abs/1809.06839
-
Altris AI Introduces Next-Generation Fluids and GA Quantification Features
Maria Znamenska, MD, PhD Ophthalmology
1 min. readAltris AI Introduces Next-Generation Fluids and GA Quantification Features
Altris AI, a pioneering force in artificial intelligence for OCT scan analysis, has unveiled additional quantification features for Fluids and Geographic Atrophy (GA) tracking on its web platform. Altris AI currently detects over 70 retina pathologies and biomarkers. However, we have decided to enhance its capabilities by adding additional Fluids and GA quantification and tracking functionalities, recognizing that eye care specialists frequently work with these conditions.
These advancements empower eye care professionals (ECPs) with cutting-edge tools for diagnosing and managing retinal diseases. By integrating AI-driven quantitative tracking and progression monitoring, Altris AI enables specialists to deliver more personalized and effective treatments, ultimately enhancing patient outcomes.
Fluids Quantification and Progression Tracking
The presence of fluids such as Intraretinal Cystoid Fluid (IRC), Diffuse Edema, Subretinal Fluid (SRF), and Serous Retinal Pigment Epithelium (RPE) Detachment are critical biomarkers for conditions like nAMD, DME, DR, and RVO. Accurate detection, quantification, and tracking of these fluids are essential for monitoring disease activity, evaluating treatment efficacy, and making informed prognoses.
We created specialized more detailed functions which detect these biomarkers for more specific and accurate tracking. The AI algorithm was additionally trained to work directly with fluids taking into account the importance of these biomarkers for accurate diagnostics.
Altris AI’s advanced algorithms, trained on millions of OCT scans, provide precise and objective fluid analysis. Each of the four fluid types is localized and color-coded for clarity. Quantitative metrics such as volume, area, and ETDRS grids (1, 3, and 6 mm) are calculated and presented in mm3 or nanoliters for comprehensive evaluation. The Progression Tracking feature offers historical trend analysis with intuitive visualizations through graphs and percentages. For instance, if Cystoid Fluid (IRC) increases in volume, ECPs can immediately identify and address the change.
Precision in Geographic Atrophy (GA) Monitoring
Recent advancements in GA treatment have led to a growing need for large-scale screening in clinical practice. However, this increased demand often means higher workloads and less time for in-depth analysis.
The platform facilitates automated detection, quantification, and tracking of GA by analyzing key biomarkers: Pigment Epithelium (RPE) atrophy, Hypertransmission, Neurosensory Retina Atrophy, and Ellipsoid Zone (EZ) disruption. These biomarkers are color-coded for easier identification.
We assess GA using three key criteria:
- Overlapping region of 3 biomarkers: Hypertransmission, RPE Atrophy, and Neurosensory Retina Atrophy (referred as the GA zone).
- The shortest distance from the Fovea center to the GA zone.
- Percentage of the GA zone covering the 1 mm, 3 mm, and 6 mm ETDRS grid areas.
We also improved the accuracy of a critical step in our AI pipeline: the fovea and central scan detection. Altris AI’s updated model is much more robust in detecting fovea zone and central scan now. Especially in cases when the center cannot be distinguished due to pathology presence or other reasons, the model is trained to analyze the whole surface and find reference locations from which a central scan could be determined. The new model can find an accurate center in 95% of cases, in other situations, it can efficiently estimate the center location (as opposed to a simple analysis flow used by ECPs where the geometrical center is selected). This advancement significantly enhances the precision of GA detection.
Further Progression Tracking enhances GA management by visualizing changes over time, supporting timely and accurate treatment decisions. By streamlining workflows and providing actionable insights, this feature helps ECPs make informed choices and potentially preserve vision in GA patients.
Dr. Maria Znamenska, MD, PhD, and a Chief Medical Officer at Altris AI, commented:
“We listened to our clients and introduced Fluids and GA tracking features. In 2025, eye care specialists will have the tools to combine their expertise with next-generation AI technology to effectively tackle conditions that threaten vision. Our formula is simple: detect, quantify, and track fluids, GA, and 70+ retina pathologies and biomarkers for better patient outcomes.”
About Altris AI
Altris AI is an artificial intelligence platform for OCT analysis that detects the widest range of retina pathologies and biomarkers on the market – more than 70. Leading the way in AI innovation, Altris AI provides transformative solutions that enhance the diagnosis, treatment, and monitoring of retinal diseases, enabling eye care professionals to deliver exceptional patient care.